Here is the Paper. Here is a post on the potential problems with randomized trials. Commentary from editors at Annals of Internal Medicine regarding the paper.
I have been asked to post on the Danish study examining if wearing masks reduces the chance of getting COVID-19. This study has been discussed at length in commentaries following publication. The study was published in the Annals of Internal Medicine (AIM) on November 18th, 2020. The editors of AIM wrote a commentary and comments followed.
The commentaries and comments following publication are worth reading. There is a great deal to learn about the conduct and interpretation of randomized trials from the variable interpretations of the study.
Here is my take on a few aspects of the trial.
Study Question.
The question is reasonable even if it is only part of the story about the potential value of wearing a mask. The researchers asked if mask wearing would reduce COVID-19. They did not ask if the mask prevents spread from people with COVID-19. (That study would be difficult to do and, perhaps, even, be unethical. Researchers would have to randomize people with COVID-19 to not wear a mask; this sort of study will not, and cannot, be done).
Design:
The trial was a randomized clinical trial; over 6000 people took part, but data were only available on 4862 due to participants dropping from the study. All people in the study received education about social distancing and other efforts to reduce COVID-19, and, then, about 1/2 were randomized to additionally receive masks. About 50% of the mask group used the masks routinely, and about 45% used masks intermittently.
Outcome measure.
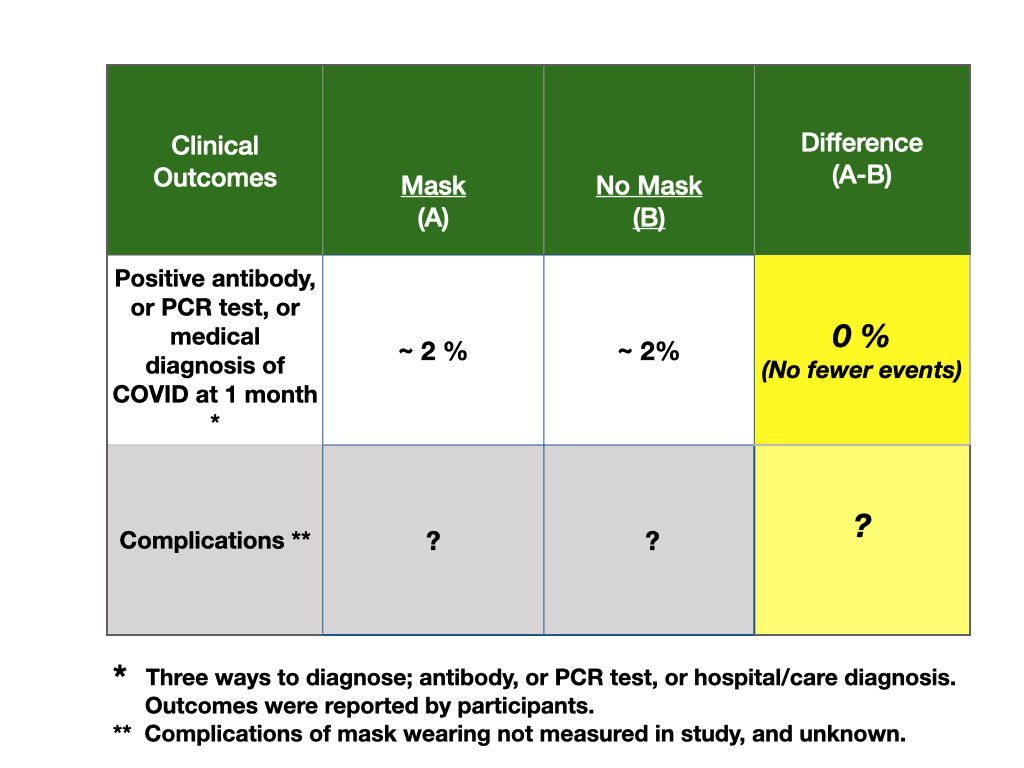
The outcome was a diagnosis of COVID-19 by one of three means; a positive antibody test, a positive PCR test, or a diagnosis at a health care setting within one month after the study started. The outcomes were self reported by participants.
Problems with the study.
This was an “unblinded” trial; this means that the participants in both groups, mask wearing and not, knew which group they were in. Knowing which study group you are in may influence a participant’s actions, such as testing behaviors. In this study, there is no assessment of the difference in how many people got tested, nor how many times they tested, between the groups. Anytime a participant knows their “treatment”, or plan of action, and when outcomes are subjective perceptions or volitional actions, failure to obscure the treatment from the participant groups may lead to bias in the measures of outcomes.
This study was an educational trial. In educational trials, a serious problem may occur when the group of people in the control portion of the trial do the same things as those in the study/intervention group. This is called, “contamination” and it occurs commonly in educational trials. The result of contamination is that there is no or little difference in the use of the study intervention, like masks, in the two groups. For example, perhaps information was being presented to the entire population, including those in the study, about how wearing a mask might help stop the spread of COVID-19. This is a common message across all countries. This may have led all participants to use masks, making the study unhelpful because there would be no comparison groups. There was no report of an assessment of mask wearing in the control group.
The study was planned to determine a 50% reduction in COVID-19 and the research team did not find this level of benefit. The chance of getting COVID-19 was low, 2%, in the month of this trial, so the difference they found between those wearing masks and those not wearing masks (1.8% versus 2.1%, difference 0.3%) was not statistically significantly different. In fact, it would have taken over 63,000 patients to detect the difference that was found.
Interpretation of study:
The potential flaws in this study make it uninterpretable. Hence, this study cannot be used to advise decision-making regarding wearing masks.
3 thoughts on “Wearing a mask for protection from COVID-19, a randomized trial.”
Patrick Walsh
It sounds like this study was not of any help, and is essentially useless. I think what’s more interesting here is that there is no comparison of complications due to the fact that wearing a mask does not have any negative health effects. The inability to study whether or not a mask helps prevent or stop the spread of COVID-19 is a moot point in my opinion (keeping in mind that it would be unethical to potentially intentionally infect people with COVID in the effort to study it). A wise man once told me: if something doesn’t have any negative effects to you or the people around you, it’s inexpensive, and it has the potential to help–what’s the harm in trying it? In this case, the inexpensive item with the potential to do good is a mask. If there’s one thing I’ve learned, it’s that things with a potential for benefit with 0 chance for harm are hard to come by. Mask wearing is one of those things, and we should take advantage of it. It is nothing more than a mild inconvenience to wear a mask when going out in public places with other people, and I don’t need a study to tell me whether or not it’s worth it to wear one. Even if I find out later that mask wearing only decreased the spread of COVID by 1%, I would consider that a success. All I had to do was wear a mask for 20 minutes at a store.
I am worker at an office and student and I have to put the mask more than eight hours a day and this is intolerable for me and many others peoples.
I see that you are not concerned by that so I please you to don’t speak about you don’t know.
If for you, “It is nothing more than a mild inconvenience to wear a mask when going out in public places for 20minutes”, lucky you are, but numbers of people have not this chance.
Many of us, workers, at office, or students, at school, have to wear a mask all day long, is more than 8 hours a day. Maybe you need some examples of what’s happening because of that ?
So : headache, reduced blood oxygenation and increased carbon dioxide in the blood (that is particularly dangerous), hypoxia (because the mask limits breathing), loss of consciousness, dizzy, decreased natural immunity, dermatological problems (pimples, eczema, dryness), death threat for some people who already have respiratory and heart problems…
More than that, children have to live with, it hinders their understanding of the world as they rely a lot on facial expressions.
I invite you to visit the site ReinfoCovid (in French), in order to understand that not everyone is comfortable with this situation.
The problem is that in the current situation everyone is responsible for the illness of others (lack of immunity) when in reality everyone is responsible for their own health (not valid for the pollution which kills millions of people every year ).
If you are struggling in the middle of the street and need help, you will be happy to have someone come and help you without worrying about touching a potential COVID carrier.
Moreover, I remind you that the first consequence of life is death. I hope for a good painless death for everyone but it is not something we need to fear.
I do not have enough vocabulary to make myself clearly understood sorry. No offense
Thank you both for your comments. My site is a site to present evidence. It is also a site to teach about science. In planning a study, the best researchers will assess the usefulness of the proposed intervention to test, estimate what a valued benefit size may be, determine a population most likely to fit the idea of the intervention, assess some level of risk and present their studies for grant/funding review.
The intervention, “mask’, is a difficult intervention to study. The researchers did a pretty good job of at least of thinking how to isolate the mask from other interventions. They then “guessed” a reasonable decline in the prevalence of infection that would make mask wearing beneficial. This guess is just that and there is no agreed upon size of benefit. However, to prove any less of a benefit than the researchers proposed would take so many people in the study it would be impossible.
So, this intervention, mask, is likely not able to be tested by a randomized trial. The randomized trial does not fit all questions, but researchers, unwittingly sometimes do not think this through. The only way to study this is to have a baseline level of infection in a full population and then uniformly have all wear masks. But, this is also untenable due to peoples preferences and lack of clear shared understanding of the value of doing studies.
In addition, individuals should make choices based on a trade-off of known benefit and known risk. Neither of these conditions is present leaving everyone and anyone to have an opinion. In a public health crises, the outcomes of interventions affect not only the wearer, but those around them. The conditions of individual shared choice are not met. Hence, both views above can be considered “correct” from their perspectives.
The passion of both who commented is treasured. Thank you. Very difficult situation, poor messaging from leaders, poor science, poor listening to people with alternative passions leaves many confused. Mask wearing is not and will never be a scientific experience, in my view. Again, thank you to both of you.

It sounds like this study was not of any help, and is essentially useless. I think what’s more interesting here is that there is no comparison of complications due to the fact that wearing a mask does not have any negative health effects. The inability to study whether or not a mask helps prevent or stop the spread of COVID-19 is a moot point in my opinion (keeping in mind that it would be unethical to potentially intentionally infect people with COVID in the effort to study it). A wise man once told me: if something doesn’t have any negative effects to you or the people around you, it’s inexpensive, and it has the potential to help–what’s the harm in trying it? In this case, the inexpensive item with the potential to do good is a mask. If there’s one thing I’ve learned, it’s that things with a potential for benefit with 0 chance for harm are hard to come by. Mask wearing is one of those things, and we should take advantage of it. It is nothing more than a mild inconvenience to wear a mask when going out in public places with other people, and I don’t need a study to tell me whether or not it’s worth it to wear one. Even if I find out later that mask wearing only decreased the spread of COVID by 1%, I would consider that a success. All I had to do was wear a mask for 20 minutes at a store.
I am worker at an office and student and I have to put the mask more than eight hours a day and this is intolerable for me and many others peoples.
I see that you are not concerned by that so I please you to don’t speak about you don’t know.
If for you, “It is nothing more than a mild inconvenience to wear a mask when going out in public places for 20minutes”, lucky you are, but numbers of people have not this chance.
Many of us, workers, at office, or students, at school, have to wear a mask all day long, is more than 8 hours a day. Maybe you need some examples of what’s happening because of that ?
So : headache, reduced blood oxygenation and increased carbon dioxide in the blood (that is particularly dangerous), hypoxia (because the mask limits breathing), loss of consciousness, dizzy, decreased natural immunity, dermatological problems (pimples, eczema, dryness), death threat for some people who already have respiratory and heart problems…
More than that, children have to live with, it hinders their understanding of the world as they rely a lot on facial expressions.
I invite you to visit the site ReinfoCovid (in French), in order to understand that not everyone is comfortable with this situation.
The problem is that in the current situation everyone is responsible for the illness of others (lack of immunity) when in reality everyone is responsible for their own health (not valid for the pollution which kills millions of people every year ).
If you are struggling in the middle of the street and need help, you will be happy to have someone come and help you without worrying about touching a potential COVID carrier.
Moreover, I remind you that the first consequence of life is death. I hope for a good painless death for everyone but it is not something we need to fear.
I do not have enough vocabulary to make myself clearly understood sorry. No offense
Thank you both for your comments. My site is a site to present evidence. It is also a site to teach about science. In planning a study, the best researchers will assess the usefulness of the proposed intervention to test, estimate what a valued benefit size may be, determine a population most likely to fit the idea of the intervention, assess some level of risk and present their studies for grant/funding review.
The intervention, “mask’, is a difficult intervention to study. The researchers did a pretty good job of at least of thinking how to isolate the mask from other interventions. They then “guessed” a reasonable decline in the prevalence of infection that would make mask wearing beneficial. This guess is just that and there is no agreed upon size of benefit. However, to prove any less of a benefit than the researchers proposed would take so many people in the study it would be impossible.
So, this intervention, mask, is likely not able to be tested by a randomized trial. The randomized trial does not fit all questions, but researchers, unwittingly sometimes do not think this through. The only way to study this is to have a baseline level of infection in a full population and then uniformly have all wear masks. But, this is also untenable due to peoples preferences and lack of clear shared understanding of the value of doing studies.
In addition, individuals should make choices based on a trade-off of known benefit and known risk. Neither of these conditions is present leaving everyone and anyone to have an opinion. In a public health crises, the outcomes of interventions affect not only the wearer, but those around them. The conditions of individual shared choice are not met. Hence, both views above can be considered “correct” from their perspectives.
The passion of both who commented is treasured. Thank you. Very difficult situation, poor messaging from leaders, poor science, poor listening to people with alternative passions leaves many confused. Mask wearing is not and will never be a scientific experience, in my view. Again, thank you to both of you.