Here is the paper. Previous blog on genetics of breast cancer. National Cancer Institute site for breast cancer.
This weeks question is from a woman who listened to my previous blog on using genetic tests to determine treatment options for breast cancer. She had received the 70-item genetic test and was told she was categorized as genetically “high-risk” based on the result, but she was also told her “clinical risk” was low. This confused her, and her physician, so she called.
Risk scores:
Low clinical risk and high genetic risk, what does this mean? After breast cancer is diagnosed, tests are done on the tissue. The tests most of you have heard about are estrogen receptors, or HER2 receptors, but there are numerous others. These tests done on the tissue, and the woman’s clinical findings (like age, number of lymph nodes with cancer, tumor size, histology, etc) sum into “risk score” groups. The higher the score, the more likely cancer will return. (Online-calculators; one linked below this blog.)
The same process is followed for the genetic tests. The genetic test she received includes 70-measures. Based on groupings of the genes, another score is given, again, the higher the score, the worse the prognosis. So, a woman can now receive two scores, one clinical and one genetic.
If the clinical and genetic scores are low (good long-term prognosis), a woman is only offered tamoxifen for treatment. If the clinical and genetic scores are high (poor long-term prognosis), chemotherapy is added to tamoxifen. While these assertions have not been tested in a randomized trial, they are commonly suggested to patients.
There is, however, no consensus on what options might be reasonable if a woman has a discrepancy between the clinical and the genetic scores. So, a randomized trial was done to attempt to answer this question (paper linked above).
The study:
In this trial, nearly 7000 women were recruited. Of these, about 40% were low/low, (clinical/genetic), and were given only tamoxifen; 10% were low/high, 25% were high/low and about 20-25% were high/high. The high/high scored women received both treatments, tamoxifen and chemotherapy.
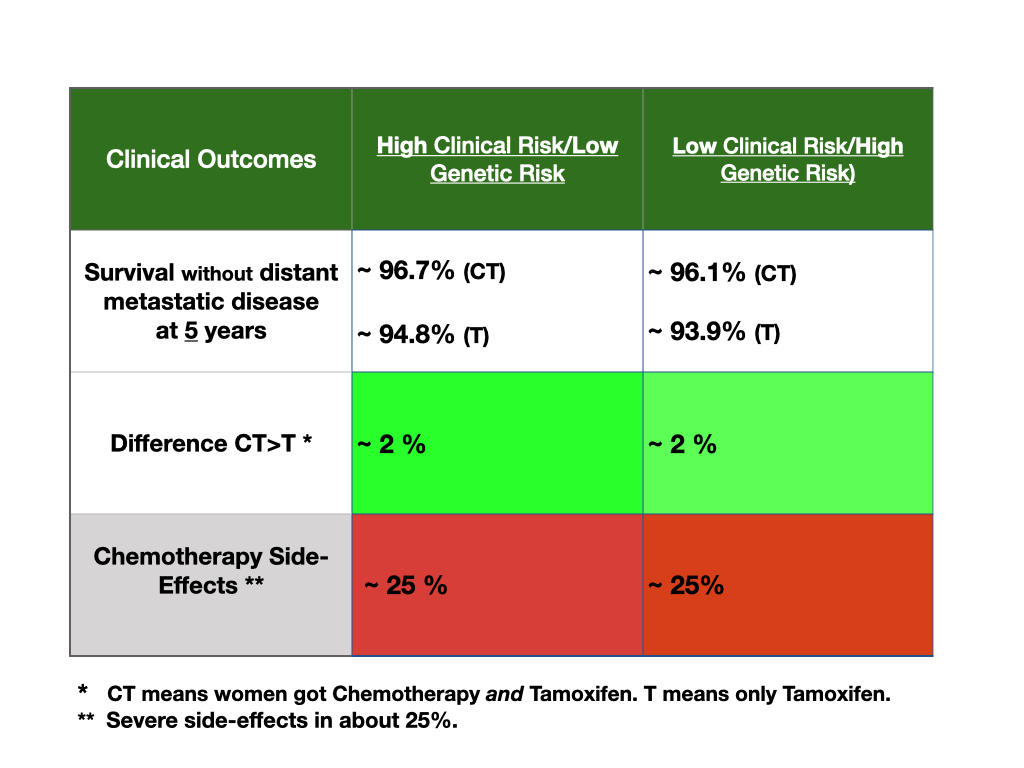
The women with discrepant risk scores were randomized to tamoxifen alone, or tamoxifen with chemotherapy. The table above shows the results.
This table has a different display than my usual tables. In this, the second and third columns include the discrepant groups. The second column shows the outcomes between chemotherapy and tamoxifen (CT) and tamoxifen alone (T) for the high risk clinical/low risk genetic scores. The third shows outcomes for the low clinical/high genetic risk group (like the lady sending in this weeks question).
Both groups of women have a good prognosis over 5 years. The main outcome measure for this trial was “surviving without distant metastatic disease” because this outcome was used to develop the risk scores. You can see that about 94-97% of women in all groups, risk profiles and treatment plans, do well.
For both discrepant groups, chemotherapy added about 2% greater chance of being well without distant metastasis. These differences, however, were not statistically significantly different. This means that the 2% difference may not be the true difference. (The overall survival of all groups were nearly the same and none were statistically significantly different or better clinically.)
Hence, it is unclear if adding chemotherapy with tamoxifen for women with discrepant clinical/genetic scores would be better for them. Chemotherapy might be 2% better in high genetic and high clinical scores, but chemotherapy also causes harm above and beyond tamoxifen treatment that is significant enough such that women might forgo any further chemotherapy in about 25%.
So, this is a tough trade-off for this woman. An added, unsure potential gain of 2%, balanced against the added potential loss of 25% for undergoing chemotherapy.
This woman decided against taking chemotherapy after seeing the data and discussing the information with her physician. She also commented that the genetic test does not seem to offer patients much help, and she lamented having the test. She noted that the overall life expectancy at 5 years for tamoxifen only treated women for both high clinical scores or high genetic scores is nearly identical at about 97%.
Given the generally good prognosis in estrogen receptor positive breast cancer, deciding to have a genetic test on breast cancer tissue, or taking chemotherapy in addition to tamoxifen is a tough clinical decision to make. Routine testing or chemotherapy treatment is difficult to presently defend.