5 thoughts on “Should I get a screening test for lung cancer?”
Robert McNutt
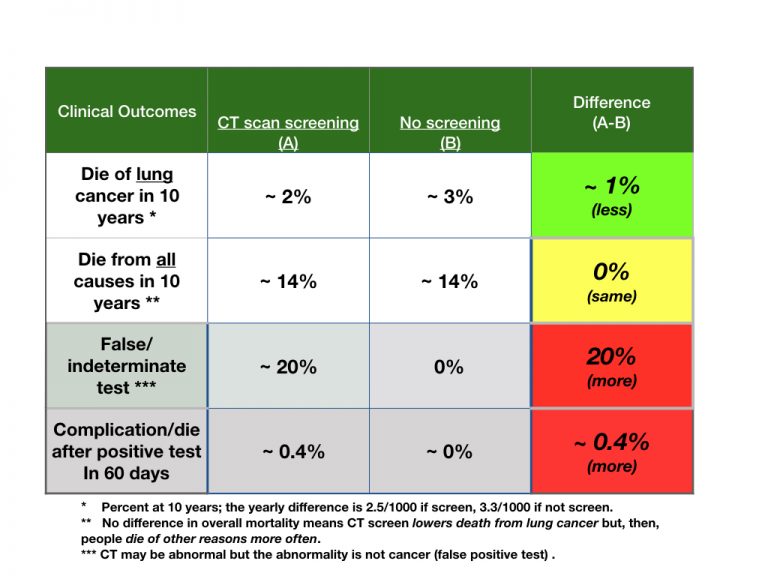
A reader wrote and asked how there can be a complication or death from the CT scan screening in the first 60 days. The CT, he said, is not a dangerous test. I thank the reader, this is a great question. Realize that the screening test, CT, finds abnormalities in the lungs. That means that if there is a concern for cancer, another test must be done. Those tests require a biopsy in lung tissue. Doing a biopsy of lung tissue is not an easy task and complications can occur. A patient of mine had a biopsy for an abnormal test and developed a collapsed lung and infection leading to him being in the hospital for over a week. The biopsy results were not cancer, but, instead, an inflammatory disease that did not need treatment. So, complications and even deaths were reported more often in the CT group in the study I linked in the post due to the complications of finding out what the CT scan was really showing. Thank you again.
When you point out that patients who did not have a CT ended up with the same life expectancy as the CT patients over 10 years, that’s a little confusing. In other words, you tell them that non-CT folks died of diabetes or other diseases, including other cancers. If I were the patient (even if I weren’t), I’d be a little confused. I’d wonder about the initial total group of patients: what did they have, how did they present, such that a doctor even contemplated doing a work-up for lung cancer? How do I fit in there such that it makes sense to give me advice based on what happened to them? I guess I’m saying, what was the medical necessity for entertaining “lung cancer” in the differential diagnosis of these patients at all? Are there indications for lung CT screening (like this one from the Mayo, which says the test is “offered”: https://www.mayoclinic.org/tests-procedures/lung-cancer-screening/about/pac-20385024 )? They “offer”, but if I don’t take their offer, the advice of MAYO CLINIC, I’d have to be a fool – and my mama didn’t raise no fool, as we say here in GA. So, I would fall into that group: 30 pack years, over age 55 (I’m 74). But for the American College of Chest Physicians, I don’t: https://www.chestnet.org/News/Press-Releases/2017/10/Am (I quit more than 15 years ago). You remember Clint Eastwood in “Dirty Harry” holding that gun in front of the guy: “How lucky do you feel today, punk?” I don’t like Luck. By the way, I really can’t remember if I’ve ever had a CT of the lungs. I’ve been bronched – not fun, even though it was flexible.
I’m just saying, if I’m the patient, I need some guidance, some security. Lung cancer is a frightening disease to me. It’s an ugly death. I might be OK about dying, but I just don’t want to die drowning in a sea of oxygen that’s not doing me any good. I have to say, I’d choose low dose chest CT every year (if that’s my risk stratum) because if there is a chance it will be positive, I need to set my house in order. It makes no difference to me that I’m ‘just as likely to die of a heart attack or something else’; I DON”T want to die of lung cancer.
So I know your philosophy is, kind of, “Here’s the information and you decide.” In this case, I’m having a problem with what each of us thinks is relevant, critical information for this guy coming to you because he is so confused. I heard Tom Friedman, the NY Times columnist, on Cuomo on CNN last night, talking about the administration’s response to coronavirus. He pointed out that some (Democratic) folks now were wanting to fight old battles in the midst of the uncertainty and frustration of this pandemic. Friedman said, “I say to these people when they bring up their information, ‘Do you want to make a POINT, or do you want to make a DIFFERENCE?'”
It looks to me like you are making a point: the data is confusing, it’s unclear, it’s 3% here and 2% there, at 10 years a lot of folks are going to be dead anyway and you might be one of them – so, it looks like a CT diagnosis of lung cancer would make no difference. But, Bob, if I’m the patient, I’m kind of begging you to make the difference. I imagine coming into your house or office and sitting down. I’m fidgeting. I have decisions to make, a life to lead. I admit that I’m somebody who would like to hear you say, “If you’re coming to me for a second opinion about just a CT scan, I’m wondering if there is not something up with you and this diagnosis and your history. What difference would it make to you, a positive or negative study? Would a positive or negative study make any difference in your current treatment for any of your other problems? Would your other active problems mean that we could NOT treat you for lung cancer if in fact your CT showed that you did have it? Let’s see if this study is applicable to you – would you have been included in it at all to make its results pertinent to your life? What are your risk factors for lung cancer? Did your doctor go over them with you? What is your doc’s thinking here? How do you feel about NOT knowing, about living in uncertainty? What about your family – how do they feel that? You know, some decisions are made just on statistics and probability. You understand those terms, right? Well, for this decision, that information is important, but you are not your statistics. You are a person, and a whole lot more than numbers.”
When I told you that when I get my cancer, I want you to be my doctor, it was not because you know how to be a Bayesian or how to calculate confidence levels or evaluate experimental design. Of course you do: that’s the price of admission into my life for this oncological drama. I would come to see you because I think you are the kind of person who became a doctor in order to make a difference in my life when I’m fast running out of, well, life itself.
I love your comments. If you have these ideas, others do as well. There are themes I will do my best to address.
First, when did you learn to think that experts matter? That just because a paper is in NEJM or that Mayo says so, it must be so? This is a fundamental flaw in judgement. In medicine, there is only the chance to chose among alternatives. The choice requires a trade-off as never does the better for you treatment come without more complications. Benefit is a difference in outcomes of disease, harm is the difference in outcomes of treatment. I can’t, Mayo can’t, no one can make that trade-off for anyone and it is offense to think otherwise. (you are not being offensive, but the theory of experts in medical decision making other than a patient is offensive, paternalistic, maternalistic nonsense). This offensiveness embodied in the idea that others should, can, do make choices for others extends to public health. I do not think our leaders did a good job of informing of the trade-offs of lockdown for the COVID-19, and the informed public should be able to weigh in on our social actions.
Second, the outcome that matters to us most is life expectancy, followed by functional well being. A smoker, and an older person, caries with them a portfolio of opportunities to die from. A smoker has a different probabilistic portfolio than a non-smoker. We really don’t get to pick and chose what we die from, we just pick and chose our actions knowing that it changes the portfolio. For smokers, they chose not only a different portfolio, but a different time line of life.
Third, screening tests are best when they “buy” life expectancy, usually happens in the young, not the old. I wish I could devise a great plan to screen for and reduce suicide, for example, as if I stop that, lots of life expectancy follows. But, if I screen at the end of the life span, no matter what I do, little benefit of screening can occur. This is the lung cancer screen issue. Yes, if you screen yearly for 3 years, your chance of “disease specific mortality for lung cancer” goes down over 10 years from 3% to 2%, a number small enough to cause many to pause. The overall mortality at 10 years is about 15% and that was the same whether people were screened or not. This means, the portfolio bought by smoking keeps relentlessly pursuing and something other than lung cancer gets you, or me.
Don’t be fooled by disease specific declines in mortality; ask for things that add life expectancy. You may not like lung cancer as a cause of death, but maybe colon cancer is worse, or a stroke, or a MI, something else in the portfolio bought by smoking. We don’t get to play those games with our life. So, I think this data does make a difference to you. You don’t have to undergo screening for lung cancer if life expectancy matters and that is really the only scientific measure of the value of services. So, tell Mayo to go jump in the lake with their recommendations if your take is that life expectancy matters most. Mayo doesn’t know anything more than anyone else. In life and medicine, there is only information of benefit and harm, and how each of us values those. Making choices like that is making a difference.
Well, Bob, we – and some others – were created for the academic dining room, or the Greenwich Village coffee house, I remember from 50 years ago! I thank you for your thinking, and especially for your passionate defense. We doctors cultivate that bland affect these days which is called “professionalism”. I’d like to point out that “professionalism” is the basis of an awful lot of side effects, morbidity, mortality, and ridiculous costs. But they sure look great in those white coats. I remember how haughty I was on the first day. Not the second, maybe, after that guy on 2Pavilion at Rush bled out on me my first night on call. I mean ON me. You were at Rush, right?
So the first thing I will ask is, how did it come about that impassioned, crucial conversations like these so rarely take place in “medicine” any more? These were the talks we had in the Commons Room at Illinois, at the School of Basic Medical Sciences, during our first year. At least, those of us who came out of the liberal arts and into medicine had those talks. (Thus, Point #1). We also had broad-minded teachers who looked at *issues* in Healthcare, and not just *problems* in medicine. Teachers and their leadership made the difference. (#2) And though they may be gone, those folks should be named because lineage – and thus, relationship and history and context – is vital. So: Dan Bloomfield, Mort Creditor, Allan Levy, John Sharpe. I worry that doctors forget they are *people*; they do not spring fully-clothed from the pages of the Washington Manuals. And – #3 – none had the leisure to talk about these concerns. “But nevertheless we persisted”, as they say. We made your type of discussion a priority because it affected both doctor and patient. Somewhere, these conversations are still going on. Just not in enough places. If they were, we would all be ‘diving deep’ below the numbers to what the numbers mean, what they represent, what the act of assigning numerical relationships truly entails.
How can you, and any other docs still in practice reading this, resurrect and externalize and face honestly that passion? I wander….
Bob, you are raising questions about the nature of “care”, about the nature of the obligations that we owe to each other as people – one of whom is sick and one of whom went to medical school. ‘Moral outrage’ and ‘burnout’ are big worries these days among doctors, and indeed among everybody. I worry from my cortex down to my pectinate line (anything past that I ain’t got much control over these days) that the *discussions* that experts have nowadays (not *conversations* between people, but *discussions* presuming knowledge and expertise) have defined away our relationships, our sense of agency, and – since many of us, myself included, don’t really understand statistical modeling and inferential thinking – our sense of competence. We plug in numbers, and so assume that *numbers* mean more than they do as we race to get ‘the right answer’. But we don’t know Bayes from booze. We much less often reason and analyze and consider contexts and preferences and intentions and purposes. But that, Bob, is what medicine is about, at least for oncologists and neurologists. OK: for any neurologist who worries about more than his wrist watch and summer home. I will let the other specialties speak for themselves if any of them are listening. In fact, I say that EVERY person who is a doctor lives and dies by what is deep in themselves and deep in the sick people who trust them. They just don’t admit it, don’t deal with it, until it’s their turn.
So I’m glad we are having this conversation. It ought to be in person, over coffee or some decent alcohol, with lots of hand-waving and eye-rolling and eyebrow-arching. Lots of laughing and interruptions and “Oh, shit, you knew that SOB too?”
Next, I absolutely do not trust so-called *experts*, but I do trust justly regarded *expertise*. I think that experts are subject to all the biases and illogicalities and ignorance that each person has who attended the classes, who wrote the dissertations (but not my own, which was faultless, of course!), who passed the Board exams given by exactly the same people who share in that ignorance, illogical thinking, and biased perspective. But expertise is different. That means you have the tools and the temperament and the ethics to analyze deeply a concern and ‘figure it out’, regardless of where it leads and how it gets there, without a hidden agenda – but perhaps with an explicit one.
Now, you have made explicit what you believe are the only ‘alternatives’: the countable number of years (or moments or days or milliseconds?) of extendable life (brainstem life? or cortical life? or reproductive life? etc.), and the countable number of unhappy events (so, maybe, episodes of milliliters of diarrhea with specific gravity of “X” per milligram of dose of medication; coughing spell of “Y” seconds resulting in drop of oxygen saturation of “Z” percent using one or another brand of pulse ox applied to the warmed right middle finger etc. etc.). And you summarize this perspective when you write: “the outcome that matters to us most is life expectancy, followed by functional well being.”
I agree with your two criteria. I just think you got the order wrong. And of course we have to agree on our definitions and how we are measuring. So, tell me what you mean by “life expectancy” and “function” and “well-being”. I think they relate to quality of life. We all have had to make that decision about when the ‘expected life’ is over and we call the code or extubate what was the person somebody loved.
We have none of us – and surely not the *experts* among us – been able to define ‘quality of life’ in nicely demarcated categories. ( https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1120435/ ). Now, I’m not saying that there are not folks who claim to be able to be able to do this, and even to digitize it in terms of, say, dollars: there is a very bright guy named Dan Ariely at Duke who makes a great case for being able to do it ( https://www.fuqua.duke.edu/faculty/dan-ariely ). But when push comes to shove (as my mom used to say) at the primary level (as experts say), “You pay your money and you take your choice.” (My maternal grandmother worked as a shill at Coney Island maybe 120 years ago, and I bet that’s how our family started saying this. You can see carnies calling this out in the old movies from the 30’s).
Even the notion of the “QALY” does not look at how the individual values their life at that moment, or for that epoch – which is what I’m interested it. The QALY is “the effects of health interventions on mortality and morbidity into a single index”. It is a “quality-adjusted life year”. And so it goes back to your measurements and preferences, which are the basis of your argument about screening.
My point is that your blog posting assumes, or seems to assume, that my measurable, physiological outcomes to your medical care are what should matter to me, not just “to the profession” or “to Medicine” or “to the insurer”. In fact, you seem to assume that you need recognize only those physiological parameters for which you have hypotheses in terms of a reductive theory of personhood. I believe that this (along with what I can gather from Theresa Hush’s postings) falls victim to the “is-ought” naturalistic fallacy: because you CAN measure what *is*, this *ought* to be what is important.
You wouldn’t tell your daughter that when she brings home the person she wants to marry, would you?
And I claim that ‘my response’ to both disease (diagnosed and undiagnosed) and therapy (both proactive and reactive) is really a negotiated judgement, an internal state, based on the valid information that you as the doctor supply in the context of my own life preferences and choices and constraints and contingencies.
I might or might not choose to have a screening CT scan. And of course, this presupposes that there is no actual immediate, ‘urgent’ (a matter of judgement, even in the AMA guide to E&M coding) medical necessity (e.g., persistent cough in a certain context, weight loss, etc.). You, and Alex Azar and Sema Verma, can say to me, “Well, we are not going to pay for it.” I get that. But the administrative, economic decision to pay for my scan is in a very different domain of thinking from,say, my fear of dying from lung cancer. You might say to me, “David, don’t be fooled. You would be a black swan in the statistical domain of CT results. You would be an outlier. Twenty years ago, in view of your smoking history and your emphysema and your funky chest XR, we all would have agreed that you should have had a CT scan. But now…. You’re going to die of *something*: you are old, buddy, and it won’t be that far off. Mortality in general might go down a bit for a fool your age if you have a scan… but especially given the risks of overdiagnosis and over-treatment, watch out! You know these doctors these days: they’d cut you open for a dollar (which is the implication of ‘overdiagnosis’ and ‘overtreatment’)… but don’t tell them that’s what we mean by ‘overtreatment’ because it would hurt their feelings plus, even worse, then we would have to actually deal with that problem, and not just at those nifty conferences sponsored by drug companies… but, truly, David, now that we have Big Data we doctors don’t think about YOUR mortality. Rather, we think about ‘mortality’ in general.”
As you say, Bob, “We don’t get to play those games with our life.” I kind of think that’s exactly the point. You are talking about ‘my life’. It is ‘my mortality.’ I am not a statistic, now, am I? I am not “a 1% drop in mortality”; I’m David Block.
I don’t really know how to argue this. We might have “a failure to communicate”, like the movie says. What if I had said to you when you finished your oncology fellowship and decided to go into ‘decision-making’, “Bob, don’t be silly! What an inefficient use of your time! You should be taking care of your patients and making money. Can you demonstrate that your second fellowship will result in exactly what you claim you need to measure and theorize about? No… you can only hope so, or presume so. Why would you make this decision about your life that you claim you have the right to do? Sure, decision-making may be interesting in theory, but we, the ASCO, measure your usefulness as an oncology fellow in terms of the total deferred mortality of the cancer population of Cook County. So, please go back to work. I’ll be checking your statistics in the morning.” You see? I can argue only from ‘well, how would you feel? see? you, too!!’
Or take those 2 young people who called you about Covid-19. (I’ve got to assume you were related to one or both of them). When you were faced with their questions, your response was “YOU do not have this disease.” Not, “A human with your presentation, assuming you have given me all the relevant information truthfully and in a uniquely interpretable and mutually comprehensible format, has this percent likelihood of having a true positive on a Covid-19 test.” No, your response was, “YOU DO NOT HAVE THIS DISEASE.” The rhetoric demonstrates your own agency, competence, and relationship. And you conferred this onto those two kids. In fact, you told them what to do. (I’m thinking you were related to them because you knew that you can tell a kid what to do, but they are going to damn well do what they please).
Why shouldn’t each and every person have that same opportunity in a relationship occasioned by a medical interaction? Don’t you want to know why I am scared to death (so to speak) of death by lung cancer? Don’t you want to know about the history of my cigarettes (I was a beatnik then, and still am), my cigars (damn, I miss them), my pipe smoking (I was an intellectual and had to look distinguished if I was to meet girls, since I clearly wasn’t a jock)? Did I give an accurate portrayal of my smoking and my cough and whatever else? Why should that 1% be so important to me? What am I afraid of? Do I not have the right to integrate that fear into my notion of ‘health’ – and isn’t the role of healthcare administration to pay attention to MY health rather than to some abstract notion of pathophysiological health, especially since this notion is biased from its 2,000 year old inception?
When I am worried about the immediacy of death, I want – I need – my doctor to hold my hand, not my numbers. Sure, you had a phone call with children. Maybe I should not judge your capacity for ‘being in the moment’ from that phone call. I’m an MD-PhD in my 70’s, with a decent IQ and an evil wit, who can still wipe his own butt; I don’t like to be infantilized. But I have to say, when I go to see MY doctor (not “a” doctor) for that peculiar moment of the sharing of information, I am going to need somebody who understands and accepts my ‘game’. Won’t we all?
So, yes, those are THE numbers. They are not MY numbers. The doctor’s moral role is to reconcile and negotiate those values together with the person in front of them. It makes the sick person feel better, regardless of the ultimate decision. And, equally important, it makes the doctor feel better, conferring moral agency, competence, and relationship.
Oh… I have no comment about the Mayo, which means of course that I do.
Sorry that I won’t be in Chicago in May. Another time.
Hi, David. Will miss bantering with you. Yes, conversation is everything and it takes, sometimes, a great deal of time to inform a person making a choice and making sure they understand the science as we best know. After informing, though, people chose differently. Some like the order you propose, go for quality over quantity, others do not. My own research in choice during fellowship showed that people are resilient and accept less than perfect outcomes for living longer. But, some do not.
Why don’t we have these conversations more often? Great question. I loved grand rounds at UNC and Tufts, they were free-for-alls and wide open sharing of ideas. I learned more epi from the conversions with Nortin, Steve, Harry, Stu Levin, than from any book. I don’t want to hypothesize why the drastic change in intellectual pursuits at the bedside because I have no special insights. We are just a different breed these days, different in goals, different in numbers, different in sub-cultures, blah, blah. But, I miss the debates and seek them when I can.

A reader wrote and asked how there can be a complication or death from the CT scan screening in the first 60 days. The CT, he said, is not a dangerous test. I thank the reader, this is a great question. Realize that the screening test, CT, finds abnormalities in the lungs. That means that if there is a concern for cancer, another test must be done. Those tests require a biopsy in lung tissue. Doing a biopsy of lung tissue is not an easy task and complications can occur. A patient of mine had a biopsy for an abnormal test and developed a collapsed lung and infection leading to him being in the hospital for over a week. The biopsy results were not cancer, but, instead, an inflammatory disease that did not need treatment. So, complications and even deaths were reported more often in the CT group in the study I linked in the post due to the complications of finding out what the CT scan was really showing. Thank you again.
A reader wrote:
When you point out that patients who did not have a CT ended up with the same life expectancy as the CT patients over 10 years, that’s a little confusing. In other words, you tell them that non-CT folks died of diabetes or other diseases, including other cancers. If I were the patient (even if I weren’t), I’d be a little confused. I’d wonder about the initial total group of patients: what did they have, how did they present, such that a doctor even contemplated doing a work-up for lung cancer? How do I fit in there such that it makes sense to give me advice based on what happened to them? I guess I’m saying, what was the medical necessity for entertaining “lung cancer” in the differential diagnosis of these patients at all? Are there indications for lung CT screening (like this one from the Mayo, which says the test is “offered”: https://www.mayoclinic.org/tests-procedures/lung-cancer-screening/about/pac-20385024 )? They “offer”, but if I don’t take their offer, the advice of MAYO CLINIC, I’d have to be a fool – and my mama didn’t raise no fool, as we say here in GA. So, I would fall into that group: 30 pack years, over age 55 (I’m 74). But for the American College of Chest Physicians, I don’t: https://www.chestnet.org/News/Press-Releases/2017/10/Am (I quit more than 15 years ago). You remember Clint Eastwood in “Dirty Harry” holding that gun in front of the guy: “How lucky do you feel today, punk?” I don’t like Luck. By the way, I really can’t remember if I’ve ever had a CT of the lungs. I’ve been bronched – not fun, even though it was flexible.
I’m just saying, if I’m the patient, I need some guidance, some security. Lung cancer is a frightening disease to me. It’s an ugly death. I might be OK about dying, but I just don’t want to die drowning in a sea of oxygen that’s not doing me any good. I have to say, I’d choose low dose chest CT every year (if that’s my risk stratum) because if there is a chance it will be positive, I need to set my house in order. It makes no difference to me that I’m ‘just as likely to die of a heart attack or something else’; I DON”T want to die of lung cancer.
So I know your philosophy is, kind of, “Here’s the information and you decide.” In this case, I’m having a problem with what each of us thinks is relevant, critical information for this guy coming to you because he is so confused. I heard Tom Friedman, the NY Times columnist, on Cuomo on CNN last night, talking about the administration’s response to coronavirus. He pointed out that some (Democratic) folks now were wanting to fight old battles in the midst of the uncertainty and frustration of this pandemic. Friedman said, “I say to these people when they bring up their information, ‘Do you want to make a POINT, or do you want to make a DIFFERENCE?'”
It looks to me like you are making a point: the data is confusing, it’s unclear, it’s 3% here and 2% there, at 10 years a lot of folks are going to be dead anyway and you might be one of them – so, it looks like a CT diagnosis of lung cancer would make no difference. But, Bob, if I’m the patient, I’m kind of begging you to make the difference. I imagine coming into your house or office and sitting down. I’m fidgeting. I have decisions to make, a life to lead. I admit that I’m somebody who would like to hear you say, “If you’re coming to me for a second opinion about just a CT scan, I’m wondering if there is not something up with you and this diagnosis and your history. What difference would it make to you, a positive or negative study? Would a positive or negative study make any difference in your current treatment for any of your other problems? Would your other active problems mean that we could NOT treat you for lung cancer if in fact your CT showed that you did have it? Let’s see if this study is applicable to you – would you have been included in it at all to make its results pertinent to your life? What are your risk factors for lung cancer? Did your doctor go over them with you? What is your doc’s thinking here? How do you feel about NOT knowing, about living in uncertainty? What about your family – how do they feel that? You know, some decisions are made just on statistics and probability. You understand those terms, right? Well, for this decision, that information is important, but you are not your statistics. You are a person, and a whole lot more than numbers.”
When I told you that when I get my cancer, I want you to be my doctor, it was not because you know how to be a Bayesian or how to calculate confidence levels or evaluate experimental design. Of course you do: that’s the price of admission into my life for this oncological drama. I would come to see you because I think you are the kind of person who became a doctor in order to make a difference in my life when I’m fast running out of, well, life itself.
That’s what I think this guy would say to you.
I love your comments. If you have these ideas, others do as well. There are themes I will do my best to address.
First, when did you learn to think that experts matter? That just because a paper is in NEJM or that Mayo says so, it must be so? This is a fundamental flaw in judgement. In medicine, there is only the chance to chose among alternatives. The choice requires a trade-off as never does the better for you treatment come without more complications. Benefit is a difference in outcomes of disease, harm is the difference in outcomes of treatment. I can’t, Mayo can’t, no one can make that trade-off for anyone and it is offense to think otherwise. (you are not being offensive, but the theory of experts in medical decision making other than a patient is offensive, paternalistic, maternalistic nonsense). This offensiveness embodied in the idea that others should, can, do make choices for others extends to public health. I do not think our leaders did a good job of informing of the trade-offs of lockdown for the COVID-19, and the informed public should be able to weigh in on our social actions.
Second, the outcome that matters to us most is life expectancy, followed by functional well being. A smoker, and an older person, caries with them a portfolio of opportunities to die from. A smoker has a different probabilistic portfolio than a non-smoker. We really don’t get to pick and chose what we die from, we just pick and chose our actions knowing that it changes the portfolio. For smokers, they chose not only a different portfolio, but a different time line of life.
Third, screening tests are best when they “buy” life expectancy, usually happens in the young, not the old. I wish I could devise a great plan to screen for and reduce suicide, for example, as if I stop that, lots of life expectancy follows. But, if I screen at the end of the life span, no matter what I do, little benefit of screening can occur. This is the lung cancer screen issue. Yes, if you screen yearly for 3 years, your chance of “disease specific mortality for lung cancer” goes down over 10 years from 3% to 2%, a number small enough to cause many to pause. The overall mortality at 10 years is about 15% and that was the same whether people were screened or not. This means, the portfolio bought by smoking keeps relentlessly pursuing and something other than lung cancer gets you, or me.
Don’t be fooled by disease specific declines in mortality; ask for things that add life expectancy. You may not like lung cancer as a cause of death, but maybe colon cancer is worse, or a stroke, or a MI, something else in the portfolio bought by smoking. We don’t get to play those games with our life. So, I think this data does make a difference to you. You don’t have to undergo screening for lung cancer if life expectancy matters and that is really the only scientific measure of the value of services. So, tell Mayo to go jump in the lake with their recommendations if your take is that life expectancy matters most. Mayo doesn’t know anything more than anyone else. In life and medicine, there is only information of benefit and harm, and how each of us values those. Making choices like that is making a difference.
Well, Bob, we – and some others – were created for the academic dining room, or the Greenwich Village coffee house, I remember from 50 years ago! I thank you for your thinking, and especially for your passionate defense. We doctors cultivate that bland affect these days which is called “professionalism”. I’d like to point out that “professionalism” is the basis of an awful lot of side effects, morbidity, mortality, and ridiculous costs. But they sure look great in those white coats. I remember how haughty I was on the first day. Not the second, maybe, after that guy on 2Pavilion at Rush bled out on me my first night on call. I mean ON me. You were at Rush, right?
So the first thing I will ask is, how did it come about that impassioned, crucial conversations like these so rarely take place in “medicine” any more? These were the talks we had in the Commons Room at Illinois, at the School of Basic Medical Sciences, during our first year. At least, those of us who came out of the liberal arts and into medicine had those talks. (Thus, Point #1). We also had broad-minded teachers who looked at *issues* in Healthcare, and not just *problems* in medicine. Teachers and their leadership made the difference. (#2) And though they may be gone, those folks should be named because lineage – and thus, relationship and history and context – is vital. So: Dan Bloomfield, Mort Creditor, Allan Levy, John Sharpe. I worry that doctors forget they are *people*; they do not spring fully-clothed from the pages of the Washington Manuals. And – #3 – none had the leisure to talk about these concerns. “But nevertheless we persisted”, as they say. We made your type of discussion a priority because it affected both doctor and patient. Somewhere, these conversations are still going on. Just not in enough places. If they were, we would all be ‘diving deep’ below the numbers to what the numbers mean, what they represent, what the act of assigning numerical relationships truly entails.
How can you, and any other docs still in practice reading this, resurrect and externalize and face honestly that passion? I wander….
Bob, you are raising questions about the nature of “care”, about the nature of the obligations that we owe to each other as people – one of whom is sick and one of whom went to medical school. ‘Moral outrage’ and ‘burnout’ are big worries these days among doctors, and indeed among everybody. I worry from my cortex down to my pectinate line (anything past that I ain’t got much control over these days) that the *discussions* that experts have nowadays (not *conversations* between people, but *discussions* presuming knowledge and expertise) have defined away our relationships, our sense of agency, and – since many of us, myself included, don’t really understand statistical modeling and inferential thinking – our sense of competence. We plug in numbers, and so assume that *numbers* mean more than they do as we race to get ‘the right answer’. But we don’t know Bayes from booze. We much less often reason and analyze and consider contexts and preferences and intentions and purposes. But that, Bob, is what medicine is about, at least for oncologists and neurologists. OK: for any neurologist who worries about more than his wrist watch and summer home. I will let the other specialties speak for themselves if any of them are listening. In fact, I say that EVERY person who is a doctor lives and dies by what is deep in themselves and deep in the sick people who trust them. They just don’t admit it, don’t deal with it, until it’s their turn.
So I’m glad we are having this conversation. It ought to be in person, over coffee or some decent alcohol, with lots of hand-waving and eye-rolling and eyebrow-arching. Lots of laughing and interruptions and “Oh, shit, you knew that SOB too?”
Next, I absolutely do not trust so-called *experts*, but I do trust justly regarded *expertise*. I think that experts are subject to all the biases and illogicalities and ignorance that each person has who attended the classes, who wrote the dissertations (but not my own, which was faultless, of course!), who passed the Board exams given by exactly the same people who share in that ignorance, illogical thinking, and biased perspective. But expertise is different. That means you have the tools and the temperament and the ethics to analyze deeply a concern and ‘figure it out’, regardless of where it leads and how it gets there, without a hidden agenda – but perhaps with an explicit one.
Now, you have made explicit what you believe are the only ‘alternatives’: the countable number of years (or moments or days or milliseconds?) of extendable life (brainstem life? or cortical life? or reproductive life? etc.), and the countable number of unhappy events (so, maybe, episodes of milliliters of diarrhea with specific gravity of “X” per milligram of dose of medication; coughing spell of “Y” seconds resulting in drop of oxygen saturation of “Z” percent using one or another brand of pulse ox applied to the warmed right middle finger etc. etc.). And you summarize this perspective when you write: “the outcome that matters to us most is life expectancy, followed by functional well being.”
I agree with your two criteria. I just think you got the order wrong. And of course we have to agree on our definitions and how we are measuring. So, tell me what you mean by “life expectancy” and “function” and “well-being”. I think they relate to quality of life. We all have had to make that decision about when the ‘expected life’ is over and we call the code or extubate what was the person somebody loved.
We have none of us – and surely not the *experts* among us – been able to define ‘quality of life’ in nicely demarcated categories. ( https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1120435/ ). Now, I’m not saying that there are not folks who claim to be able to be able to do this, and even to digitize it in terms of, say, dollars: there is a very bright guy named Dan Ariely at Duke who makes a great case for being able to do it ( https://www.fuqua.duke.edu/faculty/dan-ariely ). But when push comes to shove (as my mom used to say) at the primary level (as experts say), “You pay your money and you take your choice.” (My maternal grandmother worked as a shill at Coney Island maybe 120 years ago, and I bet that’s how our family started saying this. You can see carnies calling this out in the old movies from the 30’s).
Even the notion of the “QALY” does not look at how the individual values their life at that moment, or for that epoch – which is what I’m interested it. The QALY is “the effects of health interventions on mortality and morbidity into a single index”. It is a “quality-adjusted life year”. And so it goes back to your measurements and preferences, which are the basis of your argument about screening.
My point is that your blog posting assumes, or seems to assume, that my measurable, physiological outcomes to your medical care are what should matter to me, not just “to the profession” or “to Medicine” or “to the insurer”. In fact, you seem to assume that you need recognize only those physiological parameters for which you have hypotheses in terms of a reductive theory of personhood. I believe that this (along with what I can gather from Theresa Hush’s postings) falls victim to the “is-ought” naturalistic fallacy: because you CAN measure what *is*, this *ought* to be what is important.
You wouldn’t tell your daughter that when she brings home the person she wants to marry, would you?
And I claim that ‘my response’ to both disease (diagnosed and undiagnosed) and therapy (both proactive and reactive) is really a negotiated judgement, an internal state, based on the valid information that you as the doctor supply in the context of my own life preferences and choices and constraints and contingencies.
I might or might not choose to have a screening CT scan. And of course, this presupposes that there is no actual immediate, ‘urgent’ (a matter of judgement, even in the AMA guide to E&M coding) medical necessity (e.g., persistent cough in a certain context, weight loss, etc.). You, and Alex Azar and Sema Verma, can say to me, “Well, we are not going to pay for it.” I get that. But the administrative, economic decision to pay for my scan is in a very different domain of thinking from,say, my fear of dying from lung cancer. You might say to me, “David, don’t be fooled. You would be a black swan in the statistical domain of CT results. You would be an outlier. Twenty years ago, in view of your smoking history and your emphysema and your funky chest XR, we all would have agreed that you should have had a CT scan. But now…. You’re going to die of *something*: you are old, buddy, and it won’t be that far off. Mortality in general might go down a bit for a fool your age if you have a scan… but especially given the risks of overdiagnosis and over-treatment, watch out! You know these doctors these days: they’d cut you open for a dollar (which is the implication of ‘overdiagnosis’ and ‘overtreatment’)… but don’t tell them that’s what we mean by ‘overtreatment’ because it would hurt their feelings plus, even worse, then we would have to actually deal with that problem, and not just at those nifty conferences sponsored by drug companies… but, truly, David, now that we have Big Data we doctors don’t think about YOUR mortality. Rather, we think about ‘mortality’ in general.”
As you say, Bob, “We don’t get to play those games with our life.” I kind of think that’s exactly the point. You are talking about ‘my life’. It is ‘my mortality.’ I am not a statistic, now, am I? I am not “a 1% drop in mortality”; I’m David Block.
I don’t really know how to argue this. We might have “a failure to communicate”, like the movie says. What if I had said to you when you finished your oncology fellowship and decided to go into ‘decision-making’, “Bob, don’t be silly! What an inefficient use of your time! You should be taking care of your patients and making money. Can you demonstrate that your second fellowship will result in exactly what you claim you need to measure and theorize about? No… you can only hope so, or presume so. Why would you make this decision about your life that you claim you have the right to do? Sure, decision-making may be interesting in theory, but we, the ASCO, measure your usefulness as an oncology fellow in terms of the total deferred mortality of the cancer population of Cook County. So, please go back to work. I’ll be checking your statistics in the morning.” You see? I can argue only from ‘well, how would you feel? see? you, too!!’
Or take those 2 young people who called you about Covid-19. (I’ve got to assume you were related to one or both of them). When you were faced with their questions, your response was “YOU do not have this disease.” Not, “A human with your presentation, assuming you have given me all the relevant information truthfully and in a uniquely interpretable and mutually comprehensible format, has this percent likelihood of having a true positive on a Covid-19 test.” No, your response was, “YOU DO NOT HAVE THIS DISEASE.” The rhetoric demonstrates your own agency, competence, and relationship. And you conferred this onto those two kids. In fact, you told them what to do. (I’m thinking you were related to them because you knew that you can tell a kid what to do, but they are going to damn well do what they please).
Why shouldn’t each and every person have that same opportunity in a relationship occasioned by a medical interaction? Don’t you want to know why I am scared to death (so to speak) of death by lung cancer? Don’t you want to know about the history of my cigarettes (I was a beatnik then, and still am), my cigars (damn, I miss them), my pipe smoking (I was an intellectual and had to look distinguished if I was to meet girls, since I clearly wasn’t a jock)? Did I give an accurate portrayal of my smoking and my cough and whatever else? Why should that 1% be so important to me? What am I afraid of? Do I not have the right to integrate that fear into my notion of ‘health’ – and isn’t the role of healthcare administration to pay attention to MY health rather than to some abstract notion of pathophysiological health, especially since this notion is biased from its 2,000 year old inception?
When I am worried about the immediacy of death, I want – I need – my doctor to hold my hand, not my numbers. Sure, you had a phone call with children. Maybe I should not judge your capacity for ‘being in the moment’ from that phone call. I’m an MD-PhD in my 70’s, with a decent IQ and an evil wit, who can still wipe his own butt; I don’t like to be infantilized. But I have to say, when I go to see MY doctor (not “a” doctor) for that peculiar moment of the sharing of information, I am going to need somebody who understands and accepts my ‘game’. Won’t we all?
So, yes, those are THE numbers. They are not MY numbers. The doctor’s moral role is to reconcile and negotiate those values together with the person in front of them. It makes the sick person feel better, regardless of the ultimate decision. And, equally important, it makes the doctor feel better, conferring moral agency, competence, and relationship.
Oh… I have no comment about the Mayo, which means of course that I do.
Sorry that I won’t be in Chicago in May. Another time.
Hi, David. Will miss bantering with you. Yes, conversation is everything and it takes, sometimes, a great deal of time to inform a person making a choice and making sure they understand the science as we best know. After informing, though, people chose differently. Some like the order you propose, go for quality over quantity, others do not. My own research in choice during fellowship showed that people are resilient and accept less than perfect outcomes for living longer. But, some do not.
Why don’t we have these conversations more often? Great question. I loved grand rounds at UNC and Tufts, they were free-for-alls and wide open sharing of ideas. I learned more epi from the conversions with Nortin, Steve, Harry, Stu Levin, than from any book. I don’t want to hypothesize why the drastic change in intellectual pursuits at the bedside because I have no special insights. We are just a different breed these days, different in goals, different in numbers, different in sub-cultures, blah, blah. But, I miss the debates and seek them when I can.
Take care during this crazy time.