4 thoughts on “Shoulder pain with partial rotator-cuff tear.”
David Block
May I please throw this more than handful of spice into your pot: https://www.ncbi.nlm.nih.gov/pubmed/27422460 ? The conclusion: “A patient’s decision to undergo surgery is influenced more by low expectations regarding the effectiveness of physical therapy than by patient symptoms or anatomic features of the rotator cuff tear. As such, patient symptoms and anatomic features of the chronic rotator cuff tear may not be the best features to use when deciding on surgical intervention.”
And this commentary on another article is very interesting. While the original paper evidently showed that surgery does better – although both conservative and surgical treatments are good, the commentator tells us that the authors of the original paper “did not fully clarify which factors are associated with a patient doing better with surgery compared with nonoperative management.” Here: https://journals.lww.com/jbjsjournal/pages/articleviewer.aspx?year=2019&issue=10020&article=00015&type=Fulltext
We have no way of knowing, therefore, at least according to this paper, into which group your “gentleman” fall. But that is crucial. Wouldn’t Bishop Bayes want to know?
And, last (for now), how certain are you of the diagnosis of “rotator cuff”? At least 20% or so of folks have ‘asymptomatic’ rotator cuff tears (in that article’s sample): MRI DIAGNOSED cuff tears. So this gentleman may have 2 or more diagnoses: the tear (which does not cause his symptoms but might be a convenient ICD-10 code) and something, say, neurological. (As a retired, cynical neurologist, I can tell you that everybody has something neurological, and that these diagnoses demand at least one, maybe more, EMG, muscle biopsy, botox injection, sleep study, and anything else I learned to do in residency, fellowship, or Caribbean cruise training. Obviously this is a bad joke. I apologize. Sometimes it just seems that way).
So, Bob, if I still practiced and had a license and insurance, I’d say I still need to see the guy and his chart, and I need to talk to him to satisfy myself and to get his construal of his disease, his sense of urgency, his expectations, his disabilities, his other medical problems if any, his propensity for risk, his willingness to actually and mindfully do physical therapy, his willingness to follow up with post-op care if that is the decision. Certainly every orthopedic surgeon would do that in order to obtain informed consent, no? But, no, I would not just send him for surgery now.
You should know this I have not practiced in 10 years, and that this posting in no way constitutes ‘medical advice’, but rather friendly advice about a hypothetical patient.
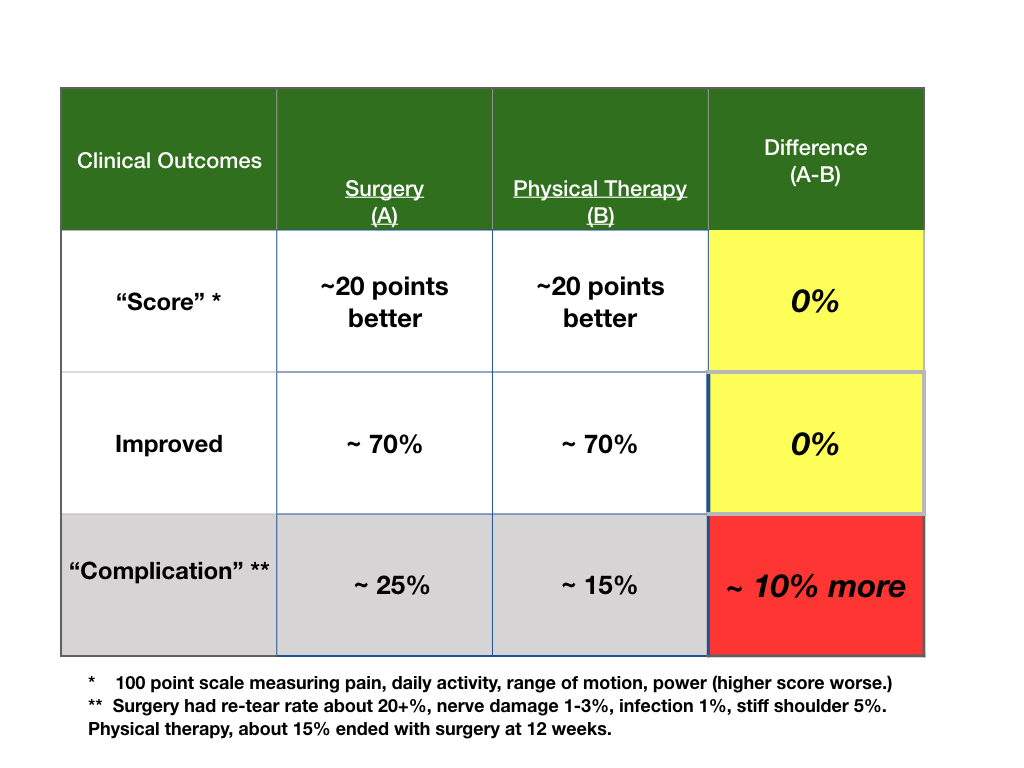
Nice comments. The state of the “art” of the science in shoulder surgery is not good. There are numerous trials with no placebo, or open label so everyone knows who is getting what, which is not adequate especially when the outcomes are subjective in nature. Each trial has a listing of the diagnoses of patients and the lists often vary in what and how much is the tear. All trials are small and impossible to tell which group or diagnosis may or may not be better. If surgery is better, most trials show small differences in scores, about 5 points, and this is likely not a clinically meaningful difference. Arthroplasty (joint replacement) has no good comparative trials or sham, which this problem begs for. Given that there are over 450,000 procedures yearly, the state of the science is just not good enough in my view.
“You’re too gentle. You didn’t mention symptoms of the surgical procedure under consideration. If he has persistent, limiting symptoms or is offered arthroscopic surgery, this is not “a tough decision” unless this 68 yo gentleman has brain fog or masochism, is afraid of his surgeon, or…. if he has symptoms, even to the extent of limiting his passion for tennis or golf or…, there is no good reason to undergo arthroscopic procedures and very good reasons not to. Furthermore, many upper extremity surgeons are shying away from arthroscopic procedures at the shoulder. There were many variations on that theme none of which were more likely to lead to gratitude from the patient than patience. Some utilized suture materials that fueled J&J product liability suits.
Arthroscopic procedures at the shoulder remain exceedingly common despite the shying away. It’s not that surgeons are practicing EBM. It’s more that they have supplanted the arthroscopic procedures with a more dangerous and lucrative procedure, arthroplasty (replacement). This has become epidemic. Soon the Fins or Swedes will do sham trials which will almost certainly echo the TKR experience.
This man needs an open conversation that leaves him informed and with agency. There is a 50% chance that whatever they’re seeing in the MRI of the symptomatic shoulder is also present in the asymptomatic shoulder.
By the time we’re 80, very few of us have rotator cuffs and it doesn’t matter. Shoulder pain afflicts about 1/3 of us in every 3 year interval. It lingers months then remits over the course of months.
Swimming and other non-violent exercises can help pass the time until remission. Remission usually leaves the patient no worse for wear.”
This man still has not decided. He admitted he did not follow PT as well as he should. He just had another MRI, so will see what he does. He was a bit shaken by the data, for sure.

May I please throw this more than handful of spice into your pot: https://www.ncbi.nlm.nih.gov/pubmed/27422460 ? The conclusion: “A patient’s decision to undergo surgery is influenced more by low expectations regarding the effectiveness of physical therapy than by patient symptoms or anatomic features of the rotator cuff tear. As such, patient symptoms and anatomic features of the chronic rotator cuff tear may not be the best features to use when deciding on surgical intervention.”
And this commentary on another article is very interesting. While the original paper evidently showed that surgery does better – although both conservative and surgical treatments are good, the commentator tells us that the authors of the original paper “did not fully clarify which factors are associated with a patient doing better with surgery compared with nonoperative management.” Here: https://journals.lww.com/jbjsjournal/pages/articleviewer.aspx?year=2019&issue=10020&article=00015&type=Fulltext
We have no way of knowing, therefore, at least according to this paper, into which group your “gentleman” fall. But that is crucial. Wouldn’t Bishop Bayes want to know?
And, last (for now), how certain are you of the diagnosis of “rotator cuff”? At least 20% or so of folks have ‘asymptomatic’ rotator cuff tears (in that article’s sample): MRI DIAGNOSED cuff tears. So this gentleman may have 2 or more diagnoses: the tear (which does not cause his symptoms but might be a convenient ICD-10 code) and something, say, neurological. (As a retired, cynical neurologist, I can tell you that everybody has something neurological, and that these diagnoses demand at least one, maybe more, EMG, muscle biopsy, botox injection, sleep study, and anything else I learned to do in residency, fellowship, or Caribbean cruise training. Obviously this is a bad joke. I apologize. Sometimes it just seems that way).
So, Bob, if I still practiced and had a license and insurance, I’d say I still need to see the guy and his chart, and I need to talk to him to satisfy myself and to get his construal of his disease, his sense of urgency, his expectations, his disabilities, his other medical problems if any, his propensity for risk, his willingness to actually and mindfully do physical therapy, his willingness to follow up with post-op care if that is the decision. Certainly every orthopedic surgeon would do that in order to obtain informed consent, no? But, no, I would not just send him for surgery now.
You should know this I have not practiced in 10 years, and that this posting in no way constitutes ‘medical advice’, but rather friendly advice about a hypothetical patient.
Nice comments. The state of the “art” of the science in shoulder surgery is not good. There are numerous trials with no placebo, or open label so everyone knows who is getting what, which is not adequate especially when the outcomes are subjective in nature. Each trial has a listing of the diagnoses of patients and the lists often vary in what and how much is the tear. All trials are small and impossible to tell which group or diagnosis may or may not be better. If surgery is better, most trials show small differences in scores, about 5 points, and this is likely not a clinically meaningful difference. Arthroplasty (joint replacement) has no good comparative trials or sham, which this problem begs for. Given that there are over 450,000 procedures yearly, the state of the science is just not good enough in my view.
A reader writes:
“You’re too gentle. You didn’t mention symptoms of the surgical procedure under consideration. If he has persistent, limiting symptoms or is offered arthroscopic surgery, this is not “a tough decision” unless this 68 yo gentleman has brain fog or masochism, is afraid of his surgeon, or…. if he has symptoms, even to the extent of limiting his passion for tennis or golf or…, there is no good reason to undergo arthroscopic procedures and very good reasons not to. Furthermore, many upper extremity surgeons are shying away from arthroscopic procedures at the shoulder. There were many variations on that theme none of which were more likely to lead to gratitude from the patient than patience. Some utilized suture materials that fueled J&J product liability suits.
Arthroscopic procedures at the shoulder remain exceedingly common despite the shying away. It’s not that surgeons are practicing EBM. It’s more that they have supplanted the arthroscopic procedures with a more dangerous and lucrative procedure, arthroplasty (replacement). This has become epidemic. Soon the Fins or Swedes will do sham trials which will almost certainly echo the TKR experience.
This man needs an open conversation that leaves him informed and with agency. There is a 50% chance that whatever they’re seeing in the MRI of the symptomatic shoulder is also present in the asymptomatic shoulder.
By the time we’re 80, very few of us have rotator cuffs and it doesn’t matter. Shoulder pain afflicts about 1/3 of us in every 3 year interval. It lingers months then remits over the course of months.
Swimming and other non-violent exercises can help pass the time until remission. Remission usually leaves the patient no worse for wear.”
This man still has not decided. He admitted he did not follow PT as well as he should. He just had another MRI, so will see what he does. He was a bit shaken by the data, for sure.