A woman read my previous blog regarding a genetic test to decide for/against adding chemotherapy to Tamoxifen (T) for her hormone responsive breast cancer. Now, during a follow-up visit with her oncologist, and nearing 5 years on T, her physician suggested she get a test called, Breast Cancer Index (BCI), to determine if she should get an additional 5-years of T. (She had previously decided against an Aromatase Inhibitor (AI) and now hoped she could stop another 5-years of all treatments). She remembered my blog and wrote to ask me to help her decide on taking the test.
I told her that the BCI had not been tested to see if it could help patients decide on further therapy. The test includes 7-individual measures and is applied to tissue from breast cancer. Cancers that are considered, “low”, on the result had fewer recurrences of cancer over nearly 10-years than those cancers graded as “high”. The data on BCI showed that a low grade score had about a 5-6% chance of recurring, intermediate grade score about 10-12% chance, and a high score, about a 30% chance. The studies that examined the BCI used tissue from other randomized trial patients, but only small percents of those patients had tissue for testing. For example, in one study, only 583 of nearly 7000 patients had tissue AND were estrogen receptor positive AND had positive lymph nodes. So, these studies are incomplete as the patient population is incomplete.
Most importantly, the BCI has never been tested for patients appropriately. An appropriate study would grade women with a BCI score prior to treatment, and, then, randomize them to further therapy, or none. The studies that matter to patients are appropriately done randomized comparison studies. If no comparison has been done, no information is useful for patient decision making.
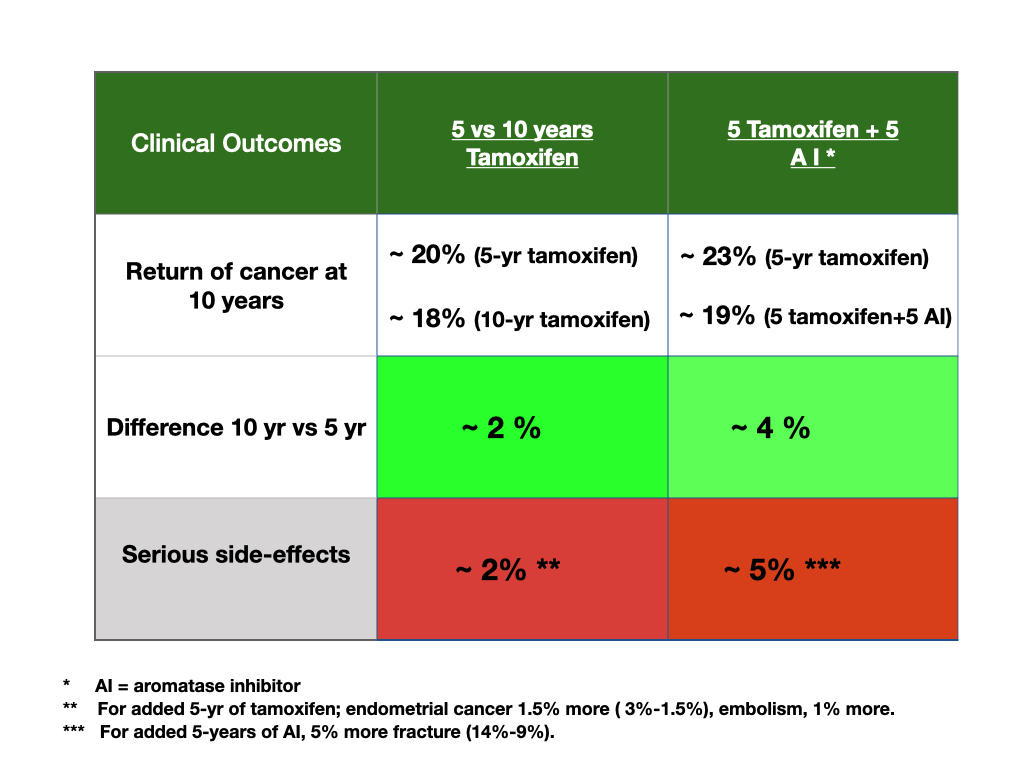
However, the patient and I were not satisfied with just stating no study had been done. So, I showed her data on extended treatment beyond 5- years of T for both added T or an AI. The table is above; green denotes better, or benefit; red denotes worse, or harm. (The usual recommendation is to add 5 more years, but a patient’s preferences for benefit and harm may influence an individual’s choice).
The reason for the recommendation to add more years of treatment is that adding either agent beyond 5-years improves overall survival over a 10- year span from about 20% to 22-24%, or about 2-4%. The patient had never seen this information. I told her she could not directly compare the added T to the added AI because these were not head to head comparisons; the results were from different studies. She then asked about the harm side. Additional years of T increases serious side-effects like endometrial cancer or blood clots about 2%, while additional years of an AI increases the harm of fractures about 5%.
She commented that adding treatment seems reasonable because the treatments adds life. To her, the harm did not seem as bad as the benefit seemed good. However, she said she did not like the side-effects of the added T compared to the added fracture risk of AI, especially because many of the fractures are not disabling, but endometrial cancer or blood clots seemed ominous to her.
She came to me to decide on a test, and decided against it. She saw that extended T or AI improved her chances of living longer even if the added chance for either was, in her words, “small”. She had previously steered clear of an AI due to fear of fracture, but the side-by-side information about the harms swayed her choice. She decided to add 5-years of an AI.
Patients are the best decision makers. They can understand studies, take into account uncertainty, and use information to make trade-offs for their care. The data affected this patient’s choice. Knowing information is better than wondering what might be best. I thank her for her consultation.
2 thoughts on “Should I take a “BCI” test to decide on 10-years of Tamoxifen?”
Patrick
Why are studies like this allowed to make it through peer review with these glaring issues? How can we push on regulatory bodies or research groups to confirm to a higher standard? It seems like the only standard here is “let’s have this study make the company creating the therapy look good so they make more money.” As a patient I don’t feel I have any power to push for better standards.
As always; great insights. It frustrates me that patients are not more involved in the choices proposed to them. Many people believe in the expertise of physicians. But, the expertise needed is a balancing of added benefit and harms of competing options for care. This is a patient’s skill not a doc’s skill. I hope that by showing patient experiences with choice that others will learn that it can be done.
On the other hand, I have become a critic of the medical literature. It is a “literature-industrial “complex system now and money matters. There are 10s of thousands of journals and studies show that about 90% of all papers submitted for publication get published somewhere. Authors can now even have their junk studies published by paying journals to publish them!
Hence, there is tons of bad data published, even in journals considered as high quality. I heard a journal editor of a major journal once claim that they hoped their journal sometimes published data that was true. I responded, all should be true. But, too many preliminary studies, too many money studies, too many competing conflicts of interest studies now dominate the landscape of publishing. I would reconfigure it all if I could and sometimes consider starting a journal of only high quality studies with critique so the public can learn. But, as for you and others frustrated like you, make sure your physician understands data, tells you about data, and gives you some assessment of the value of the data. This is especially crucial for decisions that affect your life and quality of life. Thank you for your comments.

Why are studies like this allowed to make it through peer review with these glaring issues? How can we push on regulatory bodies or research groups to confirm to a higher standard? It seems like the only standard here is “let’s have this study make the company creating the therapy look good so they make more money.” As a patient I don’t feel I have any power to push for better standards.
As always; great insights. It frustrates me that patients are not more involved in the choices proposed to them. Many people believe in the expertise of physicians. But, the expertise needed is a balancing of added benefit and harms of competing options for care. This is a patient’s skill not a doc’s skill. I hope that by showing patient experiences with choice that others will learn that it can be done.
On the other hand, I have become a critic of the medical literature. It is a “literature-industrial “complex system now and money matters. There are 10s of thousands of journals and studies show that about 90% of all papers submitted for publication get published somewhere. Authors can now even have their junk studies published by paying journals to publish them!
Hence, there is tons of bad data published, even in journals considered as high quality. I heard a journal editor of a major journal once claim that they hoped their journal sometimes published data that was true. I responded, all should be true. But, too many preliminary studies, too many money studies, too many competing conflicts of interest studies now dominate the landscape of publishing. I would reconfigure it all if I could and sometimes consider starting a journal of only high quality studies with critique so the public can learn. But, as for you and others frustrated like you, make sure your physician understands data, tells you about data, and gives you some assessment of the value of the data. This is especially crucial for decisions that affect your life and quality of life. Thank you for your comments.