Bob: This patient struggled with the difficulty of the choices he faced. He wrote a beautiful, thoughtful comment that may help others. For sure, it is difficult to make a choice when the consequences are frightening. People tend to want to try everything they can to stave off adverse clinical outcomes. But, this is an impossible task; all medical decisions are trade-offs. There is never a situation that provides only benefit and no harm; a treatment or plan that may be better from a disease standpoint will invariably be worse on some other aspect of your health due to treatment complications. This is evident with the choice for surgery for early stage prostate cancer. The patient’s comments follow. I thank him.
Patient: “I have been trying to understand why the process of my choosing what to do is so difficult. I think that it has to do with how most people generally deal with their mortality. Even when older, if we are basically healthy, we usually go about our days without thinking about the coming end, although of course we know it is inevitable. Some of us work hard at staying healthy through exercise, diet, sharing time with family and friends, working, creating, and so on. But then it happens that we have some health issues and get tests that indicate we might have a problem which could lead to our dying earlier than we expected. Often then there is also a choice of what we might do to push this predicated time out a ways. Dealing with the risks of doing nothing, or doing something that may not work, somehow does not play well with the former happy indifference to our mortality. Moreover, we also have to choose what to do based on the quality of life that we want. This is much too complicated a decision for a normal brain, even one like mine that has trained to do some pretty complicated things. I think my wife’s training in disease management, epidemiology, and one health actually equips her better for this decision process than my training and experiences have equipped me.
Anyway, we have decided that we will not be pursuing surgery soon, if ever. Even the less invasive hemiablation that I formerly thought was a good choice seems not so great now. The lack of data on its outcome is disappointing. Moreover, while I do think my doctor in DC is probably very good at using the robotic surgery techniques he uses, it is discouraging that the techniques have not greatly improved the consequences of the surgery, and that it cannot be more targeted to reduce the cancerous areas instead of using a radical approach that tries to remove or kill everything”.
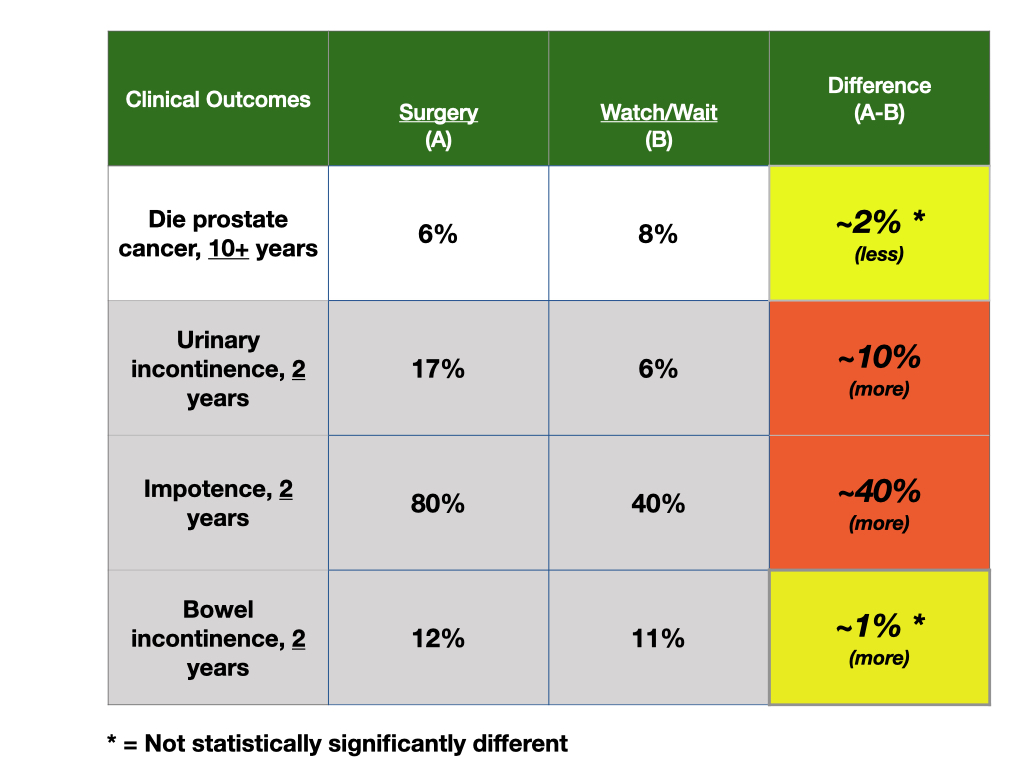
Bob: The following is a report of a trial comparing observation, versus surgery, versus radiation therapy. 1,643 randomized. Bottom line, the prostate cancer outcomes such as overall mortality, prostate cancer specific mortality do not differ between the groups. The differences are in complications; surgery more incontinence, more impotence; radiation, more bowel problems. In the observation group, with surveillance using PSA, over 50% had some intervention. [https://www.cancer.gov/types/prostate/hp/prostate-treatment-pdq].
“In the ProtecT trial (NCT02044172 and ISRCTN20141297), 82,429 men were screened with PSA testing, and 2,664 were diagnosed with clinically localized prostate cancer, of whom 1,643 (median age 62 years, range 50–69 years) consented to a randomly assigned comparison of active monitoring, radical prostatectomy (nerve-sparing when possible), or external-beam 3-dimensional (3D) conformal radiation therapy (74 Gy in 37 fractions). The primary endpoint was prostate cancer–specific mortality.[19]
With a median follow-up of 10 years, there were 17 deaths from prostate cancer, with no statistically significant differences among the three study arms (P = .48). The 10-year prostate cancer–specific survival rates were 98.8% in the active monitoring arm, 99.0% in the radical prostatectomy arm, and 99.6% in the radiation therapy arm.[19][Level of evidence: 1iiA]
Likewise, all-cause mortality was nearly identical in all three study arms: 10.9 deaths in the active monitoring arm, 10.1 in the radical prostatectomy arm, and 10.3 in the radiation therapy arm per 1,000 person-years (P = .87).[19][Level of evidence: 1iiB]
There were statistically significant differences in progression to metastatic disease among the treatment arms (active monitoring, 33/545; radical prostatectomy, 13/553; radiation therapy, 16/545) that began to emerge after 4 years, but these differences had not translated into any difference in mortality at the 10-year follow-up. Over the course of 10 years, 52% of the patients required active intervention.
As expected, there were substantial differences in patient-reported outcomes among the three management approaches.[38][Level of evidence: 1iiC] A sub-study of patient-reported outcomes up to 6 years after randomization included the following:
Men in the radical prostatectomy study arm had substantial rates of urinary incontinence (e.g., using one or more absorbent pads qd was reported by 46% at 6 months and by 17% at year 6) with very little incontinence in the other two study arms.
Sexual function was also worse in the radical prostatectomy group (e.g., at 6 months, 12% of men reported erections firm enough for intercourse versus 22% in the radiation therapy arm and 52% in the active monitoring arm).
Bowel function, however, was worse in the radiation therapy arm (e.g., about 5% reported bloody stools at least half the time at 2 years and beyond vs. none in the radical prostatectomy and active-monitoring study arms).”

A patient commented.
Bob: This patient struggled with the difficulty of the choices he faced. He wrote a beautiful, thoughtful comment that may help others. For sure, it is difficult to make a choice when the consequences are frightening. People tend to want to try everything they can to stave off adverse clinical outcomes. But, this is an impossible task; all medical decisions are trade-offs. There is never a situation that provides only benefit and no harm; a treatment or plan that may be better from a disease standpoint will invariably be worse on some other aspect of your health due to treatment complications. This is evident with the choice for surgery for early stage prostate cancer. The patient’s comments follow. I thank him.
Patient: “I have been trying to understand why the process of my choosing what to do is so difficult. I think that it has to do with how most people generally deal with their mortality. Even when older, if we are basically healthy, we usually go about our days without thinking about the coming end, although of course we know it is inevitable. Some of us work hard at staying healthy through exercise, diet, sharing time with family and friends, working, creating, and so on. But then it happens that we have some health issues and get tests that indicate we might have a problem which could lead to our dying earlier than we expected. Often then there is also a choice of what we might do to push this predicated time out a ways. Dealing with the risks of doing nothing, or doing something that may not work, somehow does not play well with the former happy indifference to our mortality. Moreover, we also have to choose what to do based on the quality of life that we want. This is much too complicated a decision for a normal brain, even one like mine that has trained to do some pretty complicated things. I think my wife’s training in disease management, epidemiology, and one health actually equips her better for this decision process than my training and experiences have equipped me.
Anyway, we have decided that we will not be pursuing surgery soon, if ever. Even the less invasive hemiablation that I formerly thought was a good choice seems not so great now. The lack of data on its outcome is disappointing. Moreover, while I do think my doctor in DC is probably very good at using the robotic surgery techniques he uses, it is discouraging that the techniques have not greatly improved the consequences of the surgery, and that it cannot be more targeted to reduce the cancerous areas instead of using a radical approach that tries to remove or kill everything”.
Bob: The following is a report of a trial comparing observation, versus surgery, versus radiation therapy. 1,643 randomized. Bottom line, the prostate cancer outcomes such as overall mortality, prostate cancer specific mortality do not differ between the groups. The differences are in complications; surgery more incontinence, more impotence; radiation, more bowel problems. In the observation group, with surveillance using PSA, over 50% had some intervention. [https://www.cancer.gov/types/prostate/hp/prostate-treatment-pdq].
“In the ProtecT trial (NCT02044172 and ISRCTN20141297), 82,429 men were screened with PSA testing, and 2,664 were diagnosed with clinically localized prostate cancer, of whom 1,643 (median age 62 years, range 50–69 years) consented to a randomly assigned comparison of active monitoring, radical prostatectomy (nerve-sparing when possible), or external-beam 3-dimensional (3D) conformal radiation therapy (74 Gy in 37 fractions). The primary endpoint was prostate cancer–specific mortality.[19]
With a median follow-up of 10 years, there were 17 deaths from prostate cancer, with no statistically significant differences among the three study arms (P = .48). The 10-year prostate cancer–specific survival rates were 98.8% in the active monitoring arm, 99.0% in the radical prostatectomy arm, and 99.6% in the radiation therapy arm.[19][Level of evidence: 1iiA]
Likewise, all-cause mortality was nearly identical in all three study arms: 10.9 deaths in the active monitoring arm, 10.1 in the radical prostatectomy arm, and 10.3 in the radiation therapy arm per 1,000 person-years (P = .87).[19][Level of evidence: 1iiB]
There were statistically significant differences in progression to metastatic disease among the treatment arms (active monitoring, 33/545; radical prostatectomy, 13/553; radiation therapy, 16/545) that began to emerge after 4 years, but these differences had not translated into any difference in mortality at the 10-year follow-up. Over the course of 10 years, 52% of the patients required active intervention.
As expected, there were substantial differences in patient-reported outcomes among the three management approaches.[38][Level of evidence: 1iiC] A sub-study of patient-reported outcomes up to 6 years after randomization included the following:
Men in the radical prostatectomy study arm had substantial rates of urinary incontinence (e.g., using one or more absorbent pads qd was reported by 46% at 6 months and by 17% at year 6) with very little incontinence in the other two study arms.
Sexual function was also worse in the radical prostatectomy group (e.g., at 6 months, 12% of men reported erections firm enough for intercourse versus 22% in the radiation therapy arm and 52% in the active monitoring arm).
Bowel function, however, was worse in the radiation therapy arm (e.g., about 5% reported bloody stools at least half the time at 2 years and beyond vs. none in the radical prostatectomy and active-monitoring study arms).”