Two readers responded to the blog saying that they gave their children the vaccine, and the side-effects were mild. One of the two suggested the estimates of side-effects of the vaccine were overstated. I thank both for their comments.
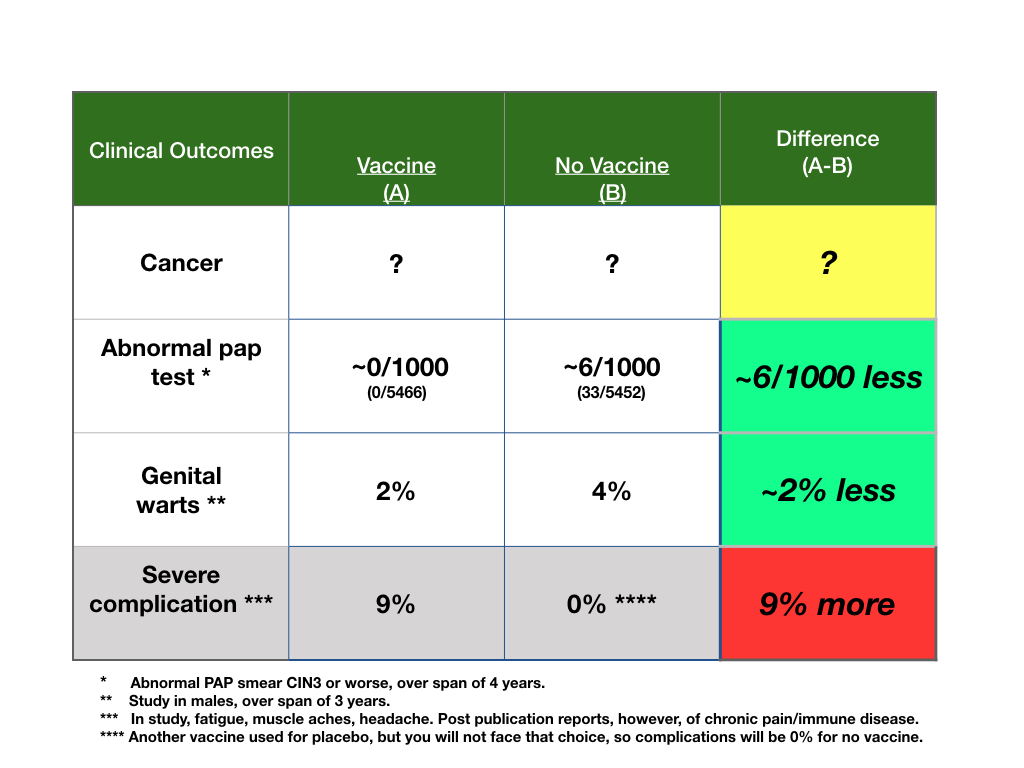
First, in response, I reported only the side-effects deemed by the researchers as “serious”. I could not find the definition of serious in the paper and I could not get the supplement where this may be described. I am sorry for that. The side-effect profile of the vaccine presented in the paper was not trivial, but it looked similar to the “placebo” vaccine. But, that is not a fair comparison. The reason, again, is that a placebo vaccine in this study is not an appropriate option for patients; if they refuse Hpv, they get nothing.
And getting nothing makes the side-effects of the Hpv vaccine more concerning. New chronic disease was seen in about 3%; ER visits, doc visits were noted in about 35%, and immune disease was noted in about 1%. The claim was that these were not related to the vaccine, but only people not getting the vaccine would have been an appropriate comparison for side-effects. Perhaps these same likelihoods of side-effects would have occurred with no vaccine comparison, but, remember, these are young people who are healthy.
More important, however, is that these comments show that the outcome we suffer or don’t suffer biases our assessment of the true potential for side-effects. All outcomes, from disease and treatment complication standpoints, are probabilistic. Just because they don’t happen to you doesn’t mean they can’t happen, and if they do, that doesn’t mean someone else will get them also. A decision should not be judged by the outcomes.
“A decision should not be judged by the outcomes”? I’m not sure I understand that assertion, especially in the context of healthcare. Do you mean we should judge our decisions by the logical processes or emotional processing by which we then act?
Why don’t you look at the “allostatic load” on a person, cumulatively and measured emotionally, mentally, and physically, in making a decision in healthcare? The “risk” from the vaccine is one time? Immediate or short term? The evaluation of the “chronic pain” and “immune disease” was… adequate? Dispositive? What is the lifetime “load” of having a positive Pap smear? Or genital warts?
All I’m saying is that the calculation of risks and benefits is by its very definition a simplification. And so often, the risks and benefits we can calculate are not the risks and benefits by which we judge our acts in the world.
Nice comments. First, every choice we make, unless it is deterministic (jump from plane without a chute, or my prostate is “gone” if I have surgery), results in events, all of them with varied probabilities. That means, to me, that after we make a choice, what happens is out of our control. I treated children with leukemia, and they chose aggressive care, universally, as without it there was certain death, and with it, some chance of life. But, some of those wonderful kids died with me at the bedside from the treatment within days to weeks. The choice was a good one, the outcome, for some, a bad one. The outcome, early treatment death, did not mean the decision was a bad one and if a person decides the decision was wrong based on that outcome, that would be unhelpful.
I don’t ever know how any person I consult with will value the potential to gain (i.e., avoid warts) and loses (i.e., chronic pain, cost of care) from a choice. I don’t know the burden of warts, but those deciding will, on some level. I think relative thinking is best. For example, is a decline in warts of 2% (from 96% chance of being well to 98% chance, given that warts can be treated) worth the potential side effects of chronic pain, even if uncertain (think of risk perception of coronovirus, for example). People will have their own senses of values to gain and lose, and the relative benefit to harm ratio gives them a target for weighing the balance when choosing. I suggest, only, that once the choice is made all we can do is to prepare for what ever events befall, good or bad. The only thing we can control is the choice, we can’t control the outcome.

Two readers responded to the blog saying that they gave their children the vaccine, and the side-effects were mild. One of the two suggested the estimates of side-effects of the vaccine were overstated. I thank both for their comments.
First, in response, I reported only the side-effects deemed by the researchers as “serious”. I could not find the definition of serious in the paper and I could not get the supplement where this may be described. I am sorry for that. The side-effect profile of the vaccine presented in the paper was not trivial, but it looked similar to the “placebo” vaccine. But, that is not a fair comparison. The reason, again, is that a placebo vaccine in this study is not an appropriate option for patients; if they refuse Hpv, they get nothing.
And getting nothing makes the side-effects of the Hpv vaccine more concerning. New chronic disease was seen in about 3%; ER visits, doc visits were noted in about 35%, and immune disease was noted in about 1%. The claim was that these were not related to the vaccine, but only people not getting the vaccine would have been an appropriate comparison for side-effects. Perhaps these same likelihoods of side-effects would have occurred with no vaccine comparison, but, remember, these are young people who are healthy.
More important, however, is that these comments show that the outcome we suffer or don’t suffer biases our assessment of the true potential for side-effects. All outcomes, from disease and treatment complication standpoints, are probabilistic. Just because they don’t happen to you doesn’t mean they can’t happen, and if they do, that doesn’t mean someone else will get them also. A decision should not be judged by the outcomes.
“A decision should not be judged by the outcomes”? I’m not sure I understand that assertion, especially in the context of healthcare. Do you mean we should judge our decisions by the logical processes or emotional processing by which we then act?
Why don’t you look at the “allostatic load” on a person, cumulatively and measured emotionally, mentally, and physically, in making a decision in healthcare? The “risk” from the vaccine is one time? Immediate or short term? The evaluation of the “chronic pain” and “immune disease” was… adequate? Dispositive? What is the lifetime “load” of having a positive Pap smear? Or genital warts?
All I’m saying is that the calculation of risks and benefits is by its very definition a simplification. And so often, the risks and benefits we can calculate are not the risks and benefits by which we judge our acts in the world.
Nice comments. First, every choice we make, unless it is deterministic (jump from plane without a chute, or my prostate is “gone” if I have surgery), results in events, all of them with varied probabilities. That means, to me, that after we make a choice, what happens is out of our control. I treated children with leukemia, and they chose aggressive care, universally, as without it there was certain death, and with it, some chance of life. But, some of those wonderful kids died with me at the bedside from the treatment within days to weeks. The choice was a good one, the outcome, for some, a bad one. The outcome, early treatment death, did not mean the decision was a bad one and if a person decides the decision was wrong based on that outcome, that would be unhelpful.
I don’t ever know how any person I consult with will value the potential to gain (i.e., avoid warts) and loses (i.e., chronic pain, cost of care) from a choice. I don’t know the burden of warts, but those deciding will, on some level. I think relative thinking is best. For example, is a decline in warts of 2% (from 96% chance of being well to 98% chance, given that warts can be treated) worth the potential side effects of chronic pain, even if uncertain (think of risk perception of coronovirus, for example). People will have their own senses of values to gain and lose, and the relative benefit to harm ratio gives them a target for weighing the balance when choosing. I suggest, only, that once the choice is made all we can do is to prepare for what ever events befall, good or bad. The only thing we can control is the choice, we can’t control the outcome.