In 2015 a randomized controlled trial (RCT) of knee replacement (TKA) versus 12-weeks of physical therapy for people with osteoarthritis (OA) was published in the New England Journal of Medicine. A quote from the authors of that paper; we are “not aware of any high-quality randomized, controlled trials of TKA …. compared to nonsurgical interventions”. This is an amazing assertion given that nearly 700,000 knee replacement surgeries are done yearly.
That RCT randomized about 100 people with “moderate to severe” OA to TKA plus 12-weeks of physical therapy versus just 12-weeks of physical therapy. Realize that the participants in this RCT knew what therapy they were getting, so this was not a “blinded” or “masked” clinical trial. Masking means that the people in a RCT should not know what treatment they are getting to reduce bias in determining the value of the treatment. Masking is the most crucial element of a scientific study, and any failure to mask – either the patient or the persons evaluating the outcome of a study – introduces bias in favor of surgical treatment. This bias is likely self evident. One of my favorite studies showing how bias works was with wine; the same wine was placed in 6 bottles and only the price of the bottle varied. People were asked to “grade the wine” on a 100-point scale. As you can imagine, the more expensive, the higher the rating. Bias is ubiquitous and in order to call a study, scientific, bias must be accounted for in the design. So, this study was biased at onset.
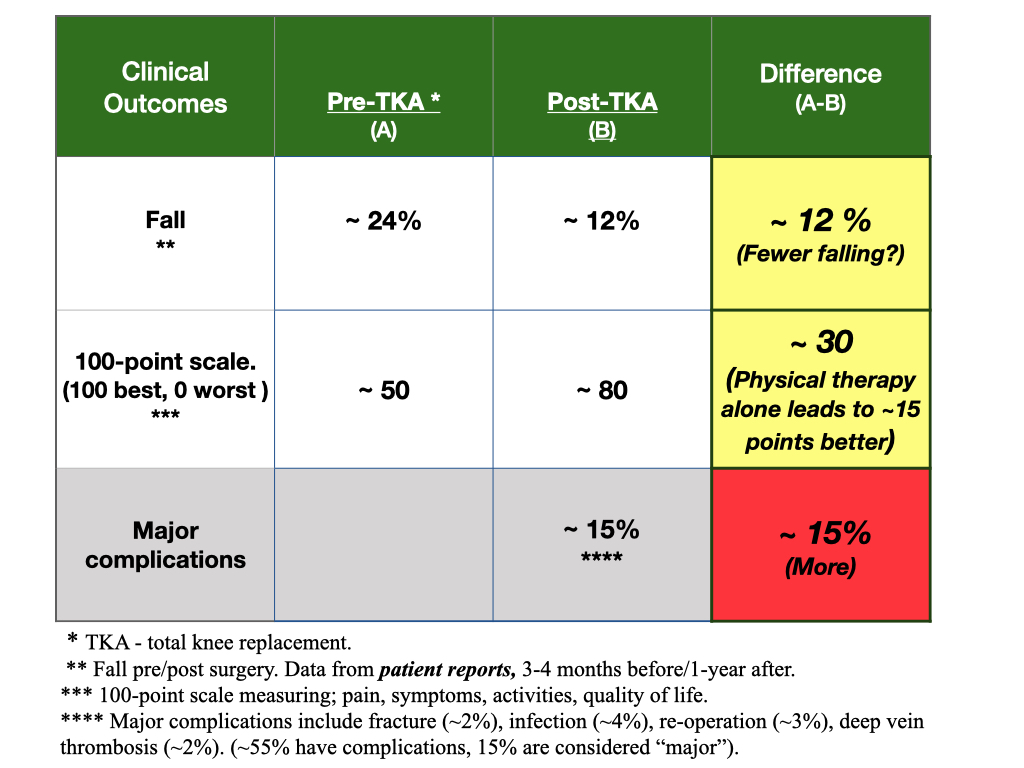
Despite the bias, the people getting TKA were only better by 16-points on a 100-point scale. The surgery group improved from a score of 50 prior to surgery to a score of 80 after (higher score better), while the physical therapy group improved from 50 prior to 66 after. So, the surgery group improved by an average of 16 points over no surgery, while nearly all in both groups improved. (Again, this score is a “subjective” measure. Subjective means that the outcome is a perception, not a physical, uniformly measurable outcome). Most importantly, 75% of the people randomized to physical therapy alone never needed TKA. Hence, despite the claim for superiority of surgery, this claim may be wrong in nearly 75%. Imagine reducing the number of surgeries for knee replacement by 75%.
This blog, however, was not motivated by this RCT and the question of whether TKA is better than physical therapy for OA on subjective outcomes. Since the RCT was not masked, the improvement in the score with surgery is likely biased, as mentioned by the authors.
This blog was motivated by a question of whether TKA improves the likelihood of a person falling. Falling is a tangible outcome measure, not a perception. However, a fall is not easy to measure, and all studies about falling before/after TKA are compromised by patient reports; which means people were asked if they fell, their falls not observed.
Also, consider that perhaps a patient who has fallen due to pain or imbalance imposed by OA may seek out surgery. In other words, perhaps falling is a trigger for surgery. Hence, falling before surgery will always be biased, and, hence, the chance of falling after TKA is destined to decline (remember, also, that physical therapy after TKA may contribute to benefit above and beyond the surgical procedure).
This destined decline is exactly what the data show; in cohorts (groups) of people getting TKA, fall rates prior to surgery compared to post surgery decline from about 20% to 10% in some studies, or from 10% to about 5% in others.
But these study results are compromised as they are based on self-reported, observational, assessments. In a systematic review of 13 studies on the benefit of knee replacement to improve balance and reduce falls, 2 studies showed higher rates of falling after surgery, 2 showed lower rates of falling, 5 showed better balance, and 7 showed no better or worse balance. These studies inform us that we don’t know if TKA benefits patients by reducing a person’s chance of falling. (Unfortunately, if people fall before surgery, 50% fall after. So, prior falls portend more likely chances for falling after TKA compared to those with TKA who did not fall prior to surgery).
The quality of evidence for TKA is poor at best and non-existent at worst. In my graph/table above, this is why I color coded the differences in both subjective and fall outcomes pre/post TKA as yellow; a warning that the data are precarious.
While there are testimonials of the benefit of TKA, these are merely case-reports, not science. In my view, the science for TKA makes the procedure unworthy for funding, or use. If this is true, why are there so many surgeries? Why do some predict a rise in TKA to over 1.5 million per year? The claim of benefit is based on opinion, not evidence-based-medicine facts. Prior to continued insurance payment, funded by all of us, appropriate, sham controlled randomized trials must be done. Without them, we will not know for sure if TKA is better for us on any outcome of importance.
2 thoughts on “Should total knee replacement (TKA) be supported by insurance?”
Patrick Walsh
How are people typically blinded in surgical studies? It seems that it would be a challenge to blind someone to a surgery since it is an easy task to tell if you have had a surgery. Another thought I had was the a possibility that those who are doing the falling are already prone to falling. In my experience, there are definitely those who are more clumsy and have worse balance to begin with. Can we control for clumsiness? How should one go about building a study for testing the fall rate due to TKA?
Howdy; you are correct. If people are falling, and if falling is a reason for the TKA, over 50% fall after the surgery. In other words, falling is a prognostic factor for outcomes after the surgery and the best predictor of future falls. Surgical studies are not difficult to “mask or blind”. In the case of TKA, patients would be randomized to getting the replacement or just the surgical process as if they were to get the replacement. They would have an incision and undergo the same post-op care with wrapped knees. Then, after, you could ask them if they got the replacement or not (called, assessment of blinding). As example, arthroscopic clean out of knees was compared to just the surgical incisions as if had and found that the outcomes were the same. Unfortunately, many surgical procedures lack high quality scientific evidence. The patient must be aware and beware of unfounded advice.

How are people typically blinded in surgical studies? It seems that it would be a challenge to blind someone to a surgery since it is an easy task to tell if you have had a surgery. Another thought I had was the a possibility that those who are doing the falling are already prone to falling. In my experience, there are definitely those who are more clumsy and have worse balance to begin with. Can we control for clumsiness? How should one go about building a study for testing the fall rate due to TKA?
Howdy; you are correct. If people are falling, and if falling is a reason for the TKA, over 50% fall after the surgery. In other words, falling is a prognostic factor for outcomes after the surgery and the best predictor of future falls. Surgical studies are not difficult to “mask or blind”. In the case of TKA, patients would be randomized to getting the replacement or just the surgical process as if they were to get the replacement. They would have an incision and undergo the same post-op care with wrapped knees. Then, after, you could ask them if they got the replacement or not (called, assessment of blinding). As example, arthroscopic clean out of knees was compared to just the surgical incisions as if had and found that the outcomes were the same. Unfortunately, many surgical procedures lack high quality scientific evidence. The patient must be aware and beware of unfounded advice.