A healthy man in his 50’s cholesterol test was “elevated” at 263. When a nurse from his physician’s office called with the result, he was told a prescription for a statin was waiting for him. Before picking it up, he wondered if the treatment would be worthwhile.
I introduced this question in a previous blog but did not disclose the the treatment. I “masked” readers to the drug hoping to teach that we should look, first, at data, not opinions, regarding the medical care offered to us. All medical tests/treatments are imperfect and a single plan must be scientifically tested against an alternative plan. The only way to make a medical decision is to compare and contrast competing plans for our care.
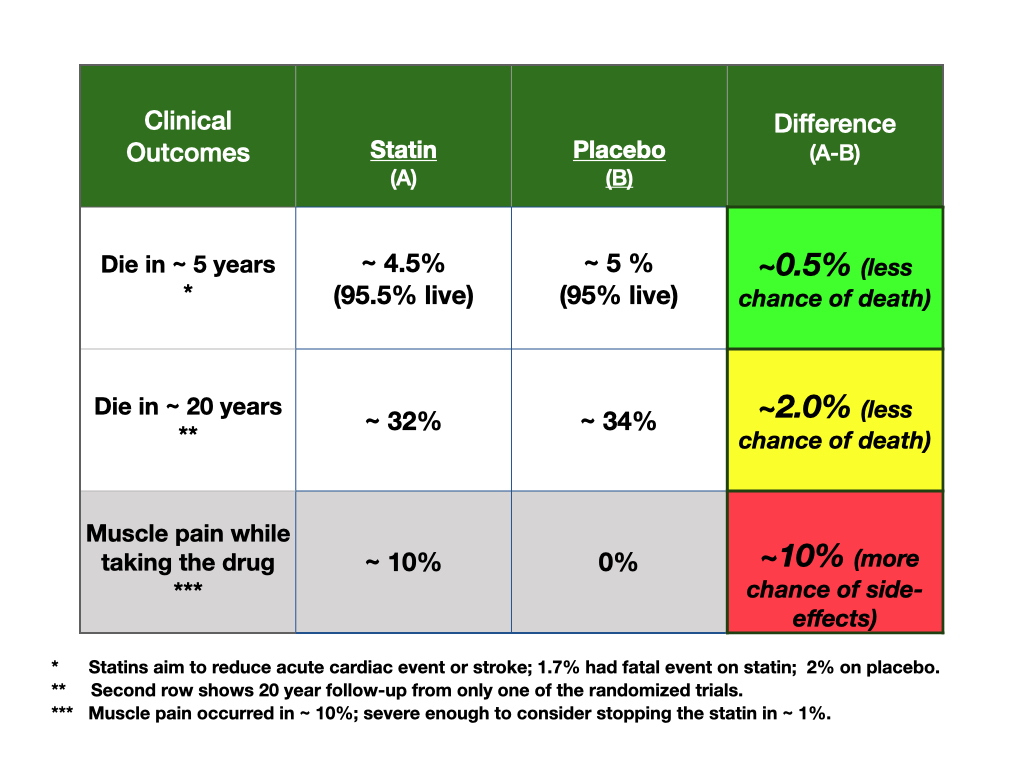
In this case, the comparison is between taking a drug, likely for life, for high cholesterol, or not. Comparisons, though, must measure outcomes that matter to us, outcomes that can be compared and contrasted. Statins are used to reduce the chance of adverse outcomes associated with a high cholesterol level. The table above is a summary of the data on the value of statins for people without pre-existing heart problems.
The table’s data is from a “meta-analysis”; 18 randomized trials have compared statins with placebos and measured cardiovascular outcomes, heart attacks and strokes. Of the 18 trials, 13 reported on the mortality difference between the compared groups. Of these 13, only one showed “strong evidence” of an improvement in overall mortality, so, 12/13 trials were uncertain for that outcome. Adding the 13 trials with mortality information, however, produced the 0.5% difference at 5 years noted in the table.
About 10% of people complained of muscle aches and pains, and only 77% of those randomized to statins complied fully with treatment. Nearly every measure of adverse cardiovascular outcomes was better with statins, but the marginal, or differences in the numbers between statins and placebo were between 0.3% to 1%.
The patient looked at the data and decided against taking the drug. For this patient, the 0.5% difference was too small. Other readers said they would take the drug at that level, but others said they would need significantly more benefit to take the drug. This is important information; all medical choices, if not emergent, should be made by those facing the choice. For some, the benefit is worth the harm, for others, not so. This is the ideal way to make a medical decision.
Presently the “system” of medicine is enamored with statins. Note that this patient’s physician called in the prescription without talking with the patient. One type of statin is the third most commonly prescribed drug with nearly 96 million prescriptions while another type is eighth on the most prescribed list.
The comments to my blog were wonderful. They showed that people will differ in how they value tests/treatments offered to them. This is why people must be the choice makers; the medical system may be over prescribing these medications to those who might not want them. And, for certain, for those who would not take this medicine, should they pay into an insurance plan that charges as if all will or should?
Another set of comments to my previous blog needs further evaluation. Some said they could not decide with the data in the table as they would need “more information”. I wondered what that other information might be, asked, but did not hear back. Evidence based medicine isthe table above. The table shows the potential consequences of a given choice, but the numbers are not enough. The patient’s preferences for benefit versus harm must be considered. Costs do not matter if someone does not want the drug, nor does any other consideration if studies have not been done to know the differences. It may be time to write a blog on the costs of medical care and how care might be better funded.