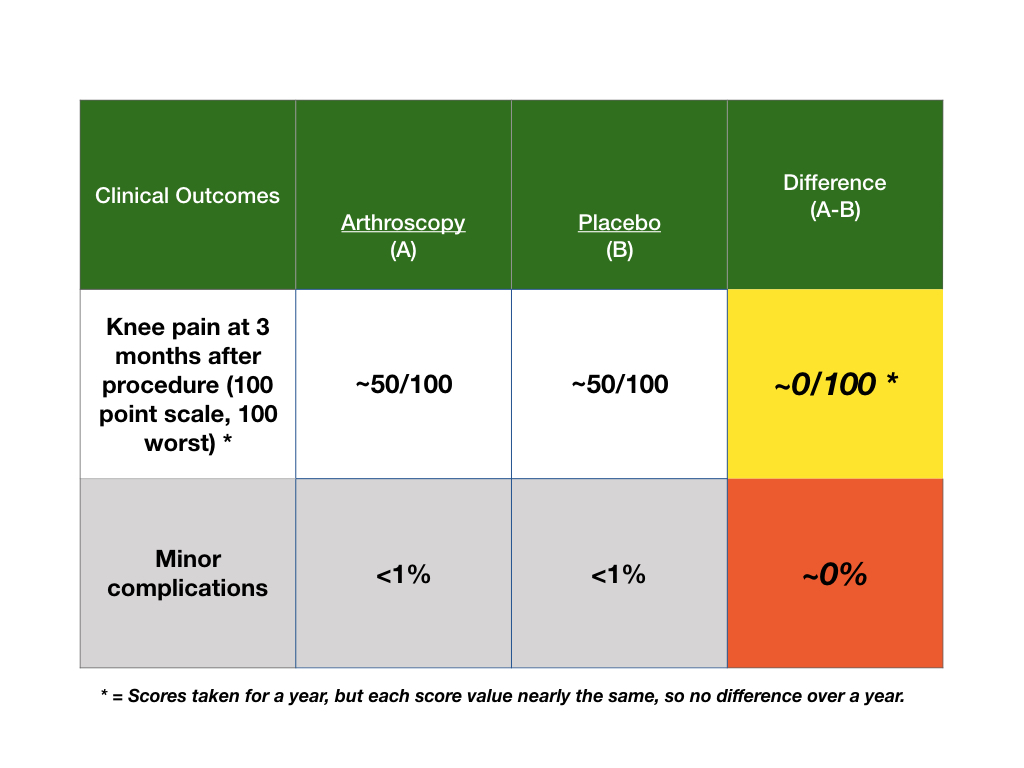
A 70 year old patient of mine called to ask if he should have an arthroscopy for arthritis of his knee. What does he need to know to decide? What would you do with the information in this table?
Well, Bob, I can see that no orthopedic surgeon is going to stop by the roadside to do CPR on you, brother.
Wasn’t there a study on sham CABG’s as well a number of years ago? I think it was about the time I had my own CABG here in GA. I can say that I felt more confident after surgery, but I don’t really know if I felt *better*. On the other hand I resolved to change my life while dealing with my urinary retention in the immediate post-op care.. Easier than psychotherapy.
So, assuming that your papers are valid, do they say more about doctors, or patients, or the culture, or the species?
Well, dear David, I hope to be driving with my wife when I need roadside assistance because she is as good as any orthopedist that I ever knew at CPR. I will say, I won’t be stopping by the roadside to do arthroscopy (would do CPR, though).
Yes, sham cardiac surgery done and pain outcomes similar to full surgery. The studies I included in this blog, like all others, were RCTs. The sham was well done with blinded outcome assessment. The physical therapy (PT) trial was balanced with PT on both sides of trial. Critiques of study were that the populations studied were not representative, but that may be a universal complaint of present day RCTs, and does not negate the fact that outcomes did not differ.
Will set up audioblog for next week. Main point will to be wary of options for care that may not benefit. Still, over 450,000 of these done in US in 2012. So, the beat goes on. Says more about doctors, perhaps; hope docs get better at informing and less good at doing. But, in my view, patients will always know best if they are informed and allowed to decide. We need to turn medicine over to them.
A reader/listener asked for more information on the “sham” surgery. First, all medical decisions need a comparison of options for care. A principle of high quality research comparisons is that neither the surgeon/researcher or the patient should know who gets what. Of course, the surgeon will know which procedure was done, but, in this case, the assessment of the outcome must be done by someone other than the surgeon. Also, the patient must not know which procedure, or drug if a drug study, they get. Studies before this sham/placebo balanced surgery showed surgery better, but the comparison option was no care and the surgeon and patient knew what they got and they assessed the outcome. This is a no-no for any research effort. This sham surgery followed the principle and assessed the patient outcomes without knowing which procedure was done.
Another listener asked if arthroscopy is good for anyone? The studies I presented were with patients who had arthritis. This surgery can be done, have had myself, for other reasons. For young people without arthritis and who suffer a torn cartilage and who have fragments left behind in their knees and have otherwise normal knees, arthroscopy may help. This is a great question as the average outcomes of a study must be modified by the specific conditions of the patient. However, given these randomized controlled trials, it is likely, in my view, that there are too many of these procedures being offered to patients. That is why I have this site. I want people to see the information so they can make their own decisions.
Excellent explanation, Bob. Given the evidence you presented, I can see no justification for surgery, given that it is painful and has inherent risks associated with anesthesia, opioid treatment post-op, and infection, not to mention the possibility of a variety of procedural and/or medication errors once one subjects oneself to medical care. Keep up the good work. I especially enjoyed listening to the audio blog.
First, thanks. Getting better at audio and hope it helps people. Plan for 200 top decisions. Also, given comments from some people who want more information in the audio, I hope to have podcast help to dive deeper into some topics.
I love your additions in comments. You are right, side-effects are not 0% likely! Also, consider the cost; $12,000 average charge. Big money for perhaps little help for patients. I support patients’ choices, but choice requires a benefit to trade-off against harm. If no benefit, I have a hard time just not saying, don’t do it. But, there are caveats and patients must go over the data with their docs. Hope you are great and thanks for the encouragement.

Well, Bob, I can see that no orthopedic surgeon is going to stop by the roadside to do CPR on you, brother.
Wasn’t there a study on sham CABG’s as well a number of years ago? I think it was about the time I had my own CABG here in GA. I can say that I felt more confident after surgery, but I don’t really know if I felt *better*. On the other hand I resolved to change my life while dealing with my urinary retention in the immediate post-op care.. Easier than psychotherapy.
So, assuming that your papers are valid, do they say more about doctors, or patients, or the culture, or the species?
Well, dear David, I hope to be driving with my wife when I need roadside assistance because she is as good as any orthopedist that I ever knew at CPR. I will say, I won’t be stopping by the roadside to do arthroscopy (would do CPR, though).
Yes, sham cardiac surgery done and pain outcomes similar to full surgery. The studies I included in this blog, like all others, were RCTs. The sham was well done with blinded outcome assessment. The physical therapy (PT) trial was balanced with PT on both sides of trial. Critiques of study were that the populations studied were not representative, but that may be a universal complaint of present day RCTs, and does not negate the fact that outcomes did not differ.
Will set up audioblog for next week. Main point will to be wary of options for care that may not benefit. Still, over 450,000 of these done in US in 2012. So, the beat goes on. Says more about doctors, perhaps; hope docs get better at informing and less good at doing. But, in my view, patients will always know best if they are informed and allowed to decide. We need to turn medicine over to them.
Thank you for your comment and best to you. Bob
A reader/listener asked for more information on the “sham” surgery. First, all medical decisions need a comparison of options for care. A principle of high quality research comparisons is that neither the surgeon/researcher or the patient should know who gets what. Of course, the surgeon will know which procedure was done, but, in this case, the assessment of the outcome must be done by someone other than the surgeon. Also, the patient must not know which procedure, or drug if a drug study, they get. Studies before this sham/placebo balanced surgery showed surgery better, but the comparison option was no care and the surgeon and patient knew what they got and they assessed the outcome. This is a no-no for any research effort. This sham surgery followed the principle and assessed the patient outcomes without knowing which procedure was done.
Another listener asked if arthroscopy is good for anyone? The studies I presented were with patients who had arthritis. This surgery can be done, have had myself, for other reasons. For young people without arthritis and who suffer a torn cartilage and who have fragments left behind in their knees and have otherwise normal knees, arthroscopy may help. This is a great question as the average outcomes of a study must be modified by the specific conditions of the patient. However, given these randomized controlled trials, it is likely, in my view, that there are too many of these procedures being offered to patients. That is why I have this site. I want people to see the information so they can make their own decisions.
Excellent explanation, Bob. Given the evidence you presented, I can see no justification for surgery, given that it is painful and has inherent risks associated with anesthesia, opioid treatment post-op, and infection, not to mention the possibility of a variety of procedural and/or medication errors once one subjects oneself to medical care. Keep up the good work. I especially enjoyed listening to the audio blog.
First, thanks. Getting better at audio and hope it helps people. Plan for 200 top decisions. Also, given comments from some people who want more information in the audio, I hope to have podcast help to dive deeper into some topics.
I love your additions in comments. You are right, side-effects are not 0% likely! Also, consider the cost; $12,000 average charge. Big money for perhaps little help for patients. I support patients’ choices, but choice requires a benefit to trade-off against harm. If no benefit, I have a hard time just not saying, don’t do it. But, there are caveats and patients must go over the data with their docs. Hope you are great and thanks for the encouragement.