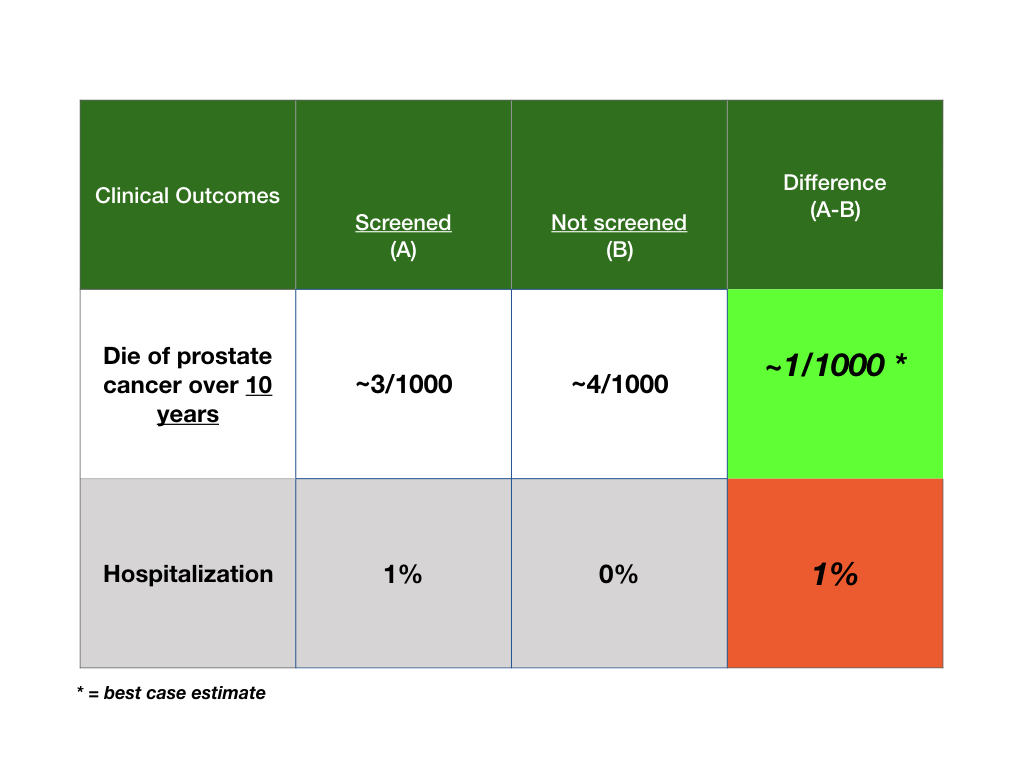
Great question. My hope/dream is that via comments we can self correct and further learn/explain nuances of the clinical questions raised by patients. In fact, there is no evidence that PSA screening benefits people over the age of 70, and, hence, in my view, it should not be offered. Of the 5 studies with over 700K people involved, only three included patients over 70 and there were not enough men in this age group to show any benefit. I told the patient this but then showed him a “best case situation” with the information in the table. Over all studies, there was no benefit but if there were, the best would be that only about 1 person in 1000 screened might benefit at 10 years. Even with this estimate the patient told me he was not taking any more tests. So the data are pertinent for all men facing this question. All the best and thank you.
This is a great start. Can you please add an additional row to the table, “Develop metastasis within 10 years”? While not as bad as death, certainly, it is a miserable disease state, so I think it would be helpful to convey what risk reduction (if any) that screening has for this outcome as well.
Dear Mike. Thanks for your comments. I did not add another outcome for several reasons. When I consult, I start with only one clinical outcome and use a best/worst case discussion. I may add another outcome (for example, when a patient with prostate cancer is contemplating surgery) if the patient is indifferent with the primary studied outcome. I did not include the “advanced disease at diagnosis” outcome because in this paper’s analysis that measure was based on a smaller sample of patients due to the lack of that measure in all randomized trials, and, also, the low confidence in the ascertainment of that outcome over 10-20 years. But, you raise a good point and I will make sure to address multiple outcomes in future audioblogs. All the best. Bob

I have a question; is this only for 72 year olds or all men?
Great question. My hope/dream is that via comments we can self correct and further learn/explain nuances of the clinical questions raised by patients. In fact, there is no evidence that PSA screening benefits people over the age of 70, and, hence, in my view, it should not be offered. Of the 5 studies with over 700K people involved, only three included patients over 70 and there were not enough men in this age group to show any benefit. I told the patient this but then showed him a “best case situation” with the information in the table. Over all studies, there was no benefit but if there were, the best would be that only about 1 person in 1000 screened might benefit at 10 years. Even with this estimate the patient told me he was not taking any more tests. So the data are pertinent for all men facing this question. All the best and thank you.
This is a great start. Can you please add an additional row to the table, “Develop metastasis within 10 years”? While not as bad as death, certainly, it is a miserable disease state, so I think it would be helpful to convey what risk reduction (if any) that screening has for this outcome as well.
Dear Mike. Thanks for your comments. I did not add another outcome for several reasons. When I consult, I start with only one clinical outcome and use a best/worst case discussion. I may add another outcome (for example, when a patient with prostate cancer is contemplating surgery) if the patient is indifferent with the primary studied outcome. I did not include the “advanced disease at diagnosis” outcome because in this paper’s analysis that measure was based on a smaller sample of patients due to the lack of that measure in all randomized trials, and, also, the low confidence in the ascertainment of that outcome over 10-20 years. But, you raise a good point and I will make sure to address multiple outcomes in future audioblogs. All the best. Bob